Fully Porous Coated Stems for Femoral Revision
William Hamilton
Jon C. Uggen
Case Presentation
A 49-year-old male presents 5 years status post a left total hip arthroplasty (THA) with significant activity-related thigh pain. His radiographs show evidence of femoral component loosening with a well-fixed cup (Fig. 119.1). Evaluation for infection was negative including a normal ESR and CRP and an isolated revision of the femoral component was indicated using an extensively porous coated diaphyseal engaging cylindrical femoral component.
Introduction
There are several surgical options available for revision of a failed femoral component in THA. These include extensively porous coated cylindrical stems, tapered Wagner type revision stems, proximal modular and nonmodular porous coated stems, second-generation cemented components, impaction allografting with cemented stems, allograft prosthetic composites, and modular oncology components. It is well recognized that the revision burden is increasing each year (1), and these technically challenging cases require a reproducible surgical approach to provide implant fixation and long-term stability. The success of extensively porous coated stems with cylindrical distal geometries for femoral revisions has been well documented (2,3,4,5,6,7,8,9,10,11,12,13,14,15,16). These stems are designed to bypass deficient proximal femoral bone and achieve diaphyseal fixation and osseointegration (17). Historically, we have considered a stem to be extensively porous coated if the coating extends over at least two-thirds of the stem length.
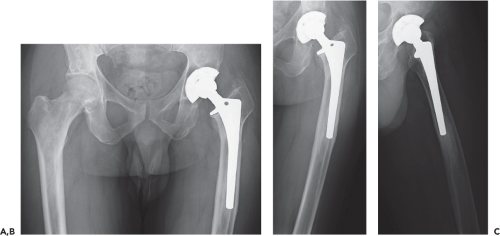 Figure 119.1. Preoperative radiographs of AP pelvis (A), AP left hip (B), and lateral left hip (C). Note the radiolucency surrounding the stem, the varus femoral remodeling, and the pedestal distally. |
In this chapter, we will utilize this case presentation to review the strategies employed when selecting a cylindrical extensively porous coated femoral stem in revision total hip surgery. The indications, contraindications, surgical planning, surgical strategies, technical pearls and pitfalls will also be discussed to help avoid potential complications faced by the surgeon. The clinical results of the currently available literature will also be reviewed.
Indications and Contraindications
Indications for revision of the femoral component include aseptic loosening, recurrent instability from malposition, component fracture, infection, severe femoral osteolysis, severe thigh pain, and the need for improved acetabular exposure (18,19,20,21,22). Careful assessment of the femoral bone stock is critical in choosing whether or not a fully porous coated femoral stem is the appropriate implant choice.
There are many classification systems used to describe femoral defects in THA (16,23,24,25). The underlining principles of these classifications rely on the surgeon’s ability to radiographically and intraoperatively assess and quantify the remaining femoral metaphyseal and diaphyseal bone stock for supportive bone. The remaining bone stock needs to provide sufficient rotational and axial support to allow for sufficient osseous integration for long-term fixation. The classification system derived from Paprosky helps guide this thought process (Table 119.1) (8,16,26).
Type I femoral defects have minimal defects confined to proximal bone, similar to what may be encountered in primary THA. Type II defects have extensive metaphyseal cancellous bone loss with minimal diaphyseal defects. Type III defects have extensive, nonsupportive, metaphyseal bone loss and diaphyseal bone loss that is subdivided into type IIIA and IIIB based on the amount of diaphyseal bone remaining for fixation. Type IIIA defects have a minimum of 4 cm of intact diaphyseal cortical bone and type IIIB defects have less than 4 cm of intact diaphyseal cortical bone. Type IV defects have extensive, nonsupportive, metaphyseal and diaphyseal bone loss. Utilizing an extensively fully porous coated stem in femoral revisions has demonstrated excellent clinical results with type I, II, and IIIA defects (Table 119.2) (2,3,4,5,6,7,8,9,10,11,12,13,14,15,16).
Table 119.1 Paprosky Classification System for Femoral Defect | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
There are limitations to extensively porous coated stems in revision THA and variables such as femoral diaphyseal quality and diameter should be considered. Sporer and Paprosky demonstrated 0% mechanical failure at average follow-up of 4.2 years in type IIIA defects with canal diameters less than 19 mm (15). When canal diameters were greater than 19 mm, the mechanical failure rate increased to 18%. A 37.5% mechanical failure rate was observed in type IV defects (15). In addition, when canal diameters are smaller than 13.5 mm, an increased rate of component fracture has been reported (27).
Preoperative radiographs should be examined to assess the difficulty in removing the current implant, the presence of retained cement or a pedestal and the presence of varus remodeling. The planned length and diameter of revision stem can be templated from these radiographs. A minimum of 4 cm but preferably 6 cm of diaphyseal bone is required to obtain reliable fixation utilizing an extensively porous coated femoral stem.
A preoperative full-length lateral radiograph is essential to determine if a bowed or straight stem is required; if a straight stem appears to penetrate the anterior femoral cortex on this view, consideration should be given to using a bowed stem. In addition to preoperative radiographic templating, ensuring the necessary equipment is available is extremely important. Commonly used equipment includes pencil tip burs, metal cutting burs, trephines, cerclage cables, oscillating saws, appropriate extraction set, hooked reverse curettes, and both morselized and strut allografts.
Preoperative templating is important to determine not only the expected size and position of the revision component, but also to determine the potential need for an extended trochanteric osteotomy (ETO). In this case, an ETO was required due to the varus remodeling of the femur and the large pedestal distally (Fig. 119.1). If an osteotomy was not performed in this case, a straight stem could exit through and damage the trochanter and abductor mechanism. The clinical success of revision THA with an extended osteotomy combined with an extensively coated revision stem has been well documented in the literature (28,29).
Surgical Technique
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


