Fragment-Specific Fixation of Distal Radius Fractures
Robert J. Medoff
DEFINITION
Fragment-specific fixation is a treatment approach for complex articular fracture patterns characterized by independent fixation of each major fracture component with an implant specific for that particular fragment (FIG 1).
Fragment-specific implants are usually low profile and have a certain degree of “spring-like” elasticity; the combination of independent fixation of multiple fragments in different planes can restore articular anatomy without the need for effective thread purchase in small periarticular fragments.
Surgical planning is extremely important to determine whether a single approach or a combination of surgical approaches is needed to visualize and fix each of the main fracture components that make up a particular injury. For distal radius fixation, a complete set of implants should be available to address any of the five primary fracture elements: the radial column, ulnar corner, volar rim, dorsal wall, and/or impacted articular fragments. In addition, identification and treatment of distal radioulnar joint (DRUJ) disruption and injuries of the ulnar column should be included.
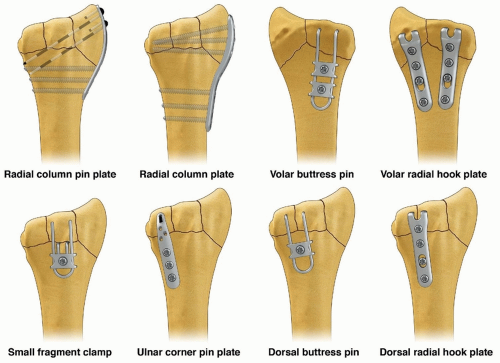
FIG 1 • Fragment-specific implants.
As a general rule, this technique avoids creation of large holes in small distal fragments, with fixation based and often triangulated to the stable ipsilateral cortex of the proximal fragment.
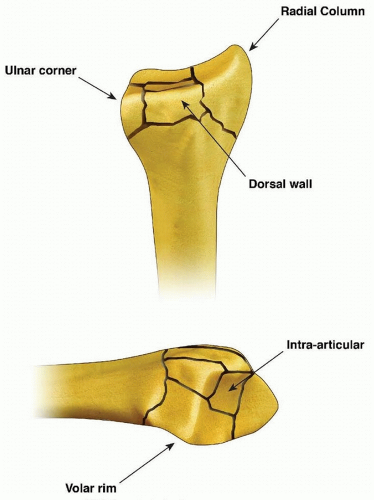 FIG 2 • Articular fracture components. |
ANATOMY
Essential Basic Anatomy
The palmar cutaneous branch of the median nerve typically lies in the subcutaneous tissue between the tendons of the flexor carpi radialis (FCR) and palmaris longus; radial-based incisions should not extend distally into a carpal tunnel approach in order to avoid injury to this nerve.
The terminal branches of the lateral antebrachial cutaneous nerve and dorsal sensory branch of the radial nerve run in the subcutaneous tissue radial to the course of the radial artery. Exposure of the radial column by elevating a radial skin and subcutaneous flap using blunt dissection from a proximal to distal direction along the surface of the first dorsal compartment tendons helps avoid injury to these structures.
The pronator quadratus inserts along the ridge at the distal flare of the radius; dissection distally should be limited to no more than 1 to 2 mm distal to the ridge to avoid compromise of the important volar carpal ligaments.
Essential Osseous Anatomy
Structurally, the wrist can be thought of in terms of three basic support columns: a radial column that includes the radial border of the distal radius and scaphoid facet, a middle column consisting of the central and ulnar part of the radial shaft and lunate facet, and an ulnar column that includes the DRUJ, the triangular fibrocartilage complex (TFCC), and the ulnar head.
The radial column fragment involves the pillar of bone along the radial border of the distal radius (FIG 2). Restoration of radial length is important to correct the axial position of the carpus, unloading deforming compressive forces that can interfere with reduction of middle column injuries. Typically, the terminal portion of the brachioradialis inserts on the base of the radial column fragment and may be a deforming force that contributes to proximal displacement of the radial column fragment. Metaphyseal comminution along the base of the radial column fragment may also contribute to radial column instability. Although not common, radial column injuries with secondary coronal fracture page or segmental comminution into the shaft proximally can be particularly unstable fracture patterns.
The volar rim of the lunate facet is a primary load-bearing structure of the articular surface. Instability of the volar rim occurs in two patterns:
In the volar instability pattern, the volar rim migrates in a proximal and volar direction resulting in secondary palmar translation of the carpus.
In the axial instability pattern of the volar rim, axial impaction of the carpus drives the volar rim into dorsiflexion, resulting in secondary axial and dorsal subluxation of the carpus.
The ulnar corner fragment involves the dorsal half of the sigmoid notch and usually includes a small dorsal ulnar corner of the articular surface of the lunate facet. This fracture component is the result of impaction of the lunate into the articular surface, causing the fragment to migrate dorsally and shorten proximally. Residual displacement of the ulnar corner may result in instability of the DRUJ as well as restriction of forearm rotation.
Dorsal wall fragmentation may be a typical finding in either dorsal bending or axial loading injuries. If displaced, this fracture component is often associated with dorsal subluxation of the carpus in addition to the typical dorsal angulation of the articular surface.
Free articular fragments may be impacted within the metaphyseal cavity and result in incongruity of the articular surface. Elevation of dorsal wall fragments allows direct access to reduction of free articular fragments.
PATHOGENESIS
Distal radius fractures are not all the same; it is a mistake to expect that a single method of treatment is uniformly effective. Careful analysis of the fragmentation pattern and the principle directions of fracture displacement can often provide useful information about the mechanism of injury and type of instability.4
Dorsal bending injuries result in extra-articular fractures with dorsal displacement (FIG 3A). Comminution of the dorsal wall and compression into metaphyseal cavity can result in dorsal instability.
Volar bending injuries result in extra-articular fractures with volar displacement (FIG 3B). Fractures with significant volar displacement are nearly always unstable and require some type of intervention to obtain and hold a reduction until union.
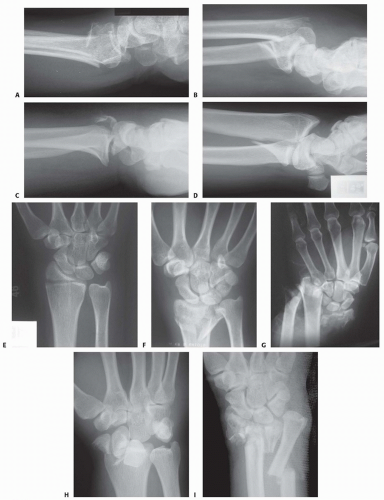
FIG 3 • Pathogenesis of dorsal radius fractures. A. Dorsal bending. B. Volar bending. C. Dorsal shear. D. Volar shear. E. Radial shear. F. Three-part articular. G. Comminuted articular. H. Carpal avulsion. I. High energy.
Dorsal shearing injuries present as fractures of the dorsal rim and are often associated with dorsal instability of the carpus (FIG 3C). These injuries often have a depressed articular fragment and may have additional radial column involvement.
Volar shearing injuries present as displaced fractures of the volar rim and result in volar instability of the carpus (FIG 3D). This pattern often has multiple articular fragments and is highly unstable. It is not usually amenable to closed methods of treatment.
Radial shearing fractures (chauffeur’s fracture) are identified by a characteristic transverse fracture line across the radial styloid that extends into the radiocarpal joint. These injuries often have more extensive chondral disruption than may be appreciated from the radiographic findings (FIG 3E).
Simple three-part fractures are usually the result of lowenergy injuries that combine a dorsal bending mechanism with some axial loading across the carpus (FIG 3F). This pattern is characterized by the presence of an ulnar corner fragment involving the dorsal portion of the sigmoid notch, a main articular fragment, and a proximal shaft fragment.
Complex articular fractures are usually the result of axial loading injuries from moderate to high-energy trauma. In addition to articular comminution, this pattern may often generate a significant defect in the metaphyseal cavity or complete disruption of the DRUJ (FIG 3G).
The avulsion/carpal instability pattern is primarily a ligamentous injury of the carpus with associated osseous avulsions of the distal radius. Bone fragments are typically small and very distal (FIG 3H).
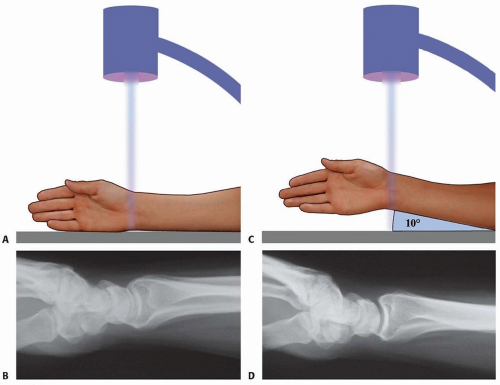
FIG 4 • A. Positioning for standard lateral radiography. B. Standard lateral radiograph. C. Positioning for 10-degree lateral radiography. D. Ten-degree lateral radiograph. Note the improved visualization of the articular surface of the base of the scaphoid facet and the entire lunate facet.
Injuries from a high-energy mechanism present as complex comminuted fractures of the articular surface with extension into the radial/ulnar shaft (FIG 3I).
IMAGING AND OTHER DIAGNOSTIC STUDIES
Posteroanterior (PA), standard lateral (FIG 4A,B), and 10-degree lateral views are routine views for radiographic evaluation of the distal radius. The 10-degree lateral view (FIG 4C,D) clearly visualizes the ulnar two-thirds of the articular surface from the base of the scaphoid facet through the entire lunate facet. Oblique views may also be helpful for evaluating the injury.
The radiographic features of distal radius fractures include the following8:
Carpal facet horizon (FIG 5A,B). This is the radiodense horizontal landmark that is used to identify the volar and dorsal rim on the PA view. If the articular surface has palmar tilt, the x-ray beam is tangential to the subchondral bone of the volar portion of the lunate facet, with the result that the carpal facet horizon identifies the volar rim. However, if the articular surface has displaced into dorsal tilt, the x-ray beam becomes tangential to the subchondral bone of the dorsal portion of the lunate facet instead, and the carpal facet horizon identifies the dorsal rim (not shown). The carpal facet horizon corresponds to the portion of the articular surface visualized on the 10-degree lateral x-ray projection.
Teardrop angle (normal 70 ± 5 degrees; FIG 5C,D). The teardrop angle is used to identify dorsiflexion of the volar
rim of the lunate facet. Depression of the teardrop angle to a value less than 45 degrees indicates that the volar rim of the lunate facet has rotated dorsally and impacted into the metaphyseal cavity (axial instability pattern of the volar rim). This may be associated with axial and dorsal subluxation of the carpus. Restoration of the teardrop angle is necessary to correct this type of malreduction.
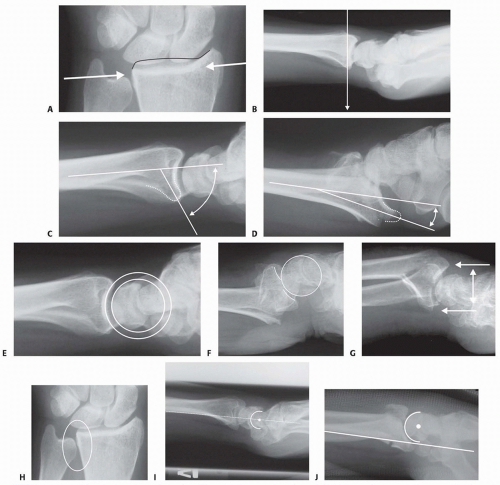
FIG 5 • A. Carpal facet horizon (arrows). Used to differentiate between the volar and dorsal rim on the PA projection. B. Origin of carpal facet horizon. The carpal facet horizon is formed by that part of the articular surface that is parallel to the x-ray beam and depends on whether the articular surface is in volar or dorsal tilt. C. Normal teardrop angle. D. Depressed teardrop angle in this case is caused by axial instability of the volar rim. E. Normal articular congruency. F. Abnormal articular congruency, indicating disruption across the volar and dorsal surfaces of the lunate facet. G. AP interval is the point-to-point distance between the corners of the dorsal and volar rim. H. DRUJ interval. I. Normal lateral carpal alignment. J. Dorsal subluxation of the carpus.
Congruency of the articular surface (FIG 5E,F). The subchondral outline of the articular surface of the distal radius is normally both congruent and concentric with the subchondral outline of the base of the lunate; a uniform joint interval should be present between the radius and lunate along the entire articular surface. When the joint interval between these articular surfaces is not uniform, discontinuity and disruption of the lunate facet has occurred.
Anteroposterior (AP) distance (normal: females 18 ± 1 mm, males 20 ± 1 mm; FIG 5G). The AP distance is the point-to-point distance from the dorsal to palmar rim of the lunate facet. It is best evaluated on the 10-degree lateral view. Widening of the AP distance implies discontinuity of the volar and dorsal portion of the lunate facet.
DRUJ interval (FIG 5H). The DRUJ interval measures the degree of apposition between the head of the ulna and the sigmoid notch (normal: 2 mm or less). This parameter is best measured with the forearm in neutral rotation. Significant widening of the DRUJ interval implies disruption of the DRUJ capsule and TFCC. Coronal malalignment of the distal radial fragment is often suggested by widening of the DRUJ interval.
Lateral carpal alignment (FIG 5I,J). On the 10-degree lateral view and with the wrist in neutral position, the rotational center of the capitate normally aligns with a line extended from the volar surface of the radial shaft. Dorsal rotation of the volar rim results in a dorsal shift of lateral carpal alignment as the carpus subluxes dorsally. This may place the flexor tendons at a mechanical disadvantage, affecting grip strength.
In addition to injury films, reassessing radiographs after reduction can be very helpful in determining the personality and specific components of a particular fracture.
Computed tomography (CT) scans allow higher resolution and definition of fracture characteristics, particularly for highly comminuted fractures. Preferably, an attempt at closed reduction before obtaining a CT scan will help limit distortion of the image. CT scans are particularly helpful for visualizing intra-articular fragments as well as DRUJ disruption and incongruity of the sigmoid notch.
Clinical evaluation of the carpus, interosseous membrane, and elbow, combined with radiographic studies when needed, should be included to identify the presence of other injuries that may affect the decision for a particular treatment.
SURGICAL MANAGEMENT
Operative Indications
General parameters
Shortening of more than 5 mm
Radial inclination of less than 15 degrees
Dorsal angulation of more than 10 degrees
Articular step-off of more than 1 to 2 mm
Depression of teardrop angle to less than 45 degrees
Volar instability
DRUJ instability
Displaced articular fractures
Young, active patients are generally less tolerant of residual deformity and malposition.
Preoperative Planning
Extra-articular fractures: multiple options
Volar plating through a volar approach
Dorsal plating through a dorsal approach
Fragment-specific fixation
Radial pin plate (TriMed, Inc., Valencia, CA) and volar buttress pin (TriMed, Inc.) fixation through a limited incision volar or standard volar approach
Radial pin plate and either an ulnar pin plate dorsally or a dorsal buttress pin through a dorsal or combined approach
Fixed-angle radial column plate using either a volar or dorsal radial column exposure
Volar hook plates with or without radial column plate using a volar approach
Intra-articular fractures: Surgical approach is based on the fragmentation pattern.
Unstable volar rim fragments require a standard volar or rarely an ulnar-based volar approach for adequate visualization.
Fixation of the radial column can be done either through a limited-incision volar radial approach (Henry), a volar approach with radial extension combined with pronation of the forearm, or a dorsal approach with radial extension combined with supination of the forearm.
Fixation of dorsal, ulnar corner, and free intra-articular fragments can be done through a dorsal approach.
Positioning
The patient is supine.
The affected arm is placed on an arm board out to the side.
C-arm
If the arm board is radiolucent, the C-arm can be brought in from the end of the arm board and images taken directly with the wrist on the arm board.
If the arm board is not radiolucent, the C-arm is brought in along the side of the table from the foot, and the arm is brought off the arm board for each image.
Operative Sequence
Initial restoration of radial column length with traction and provisional trans-styloid pin fixation can be helpful to hold the carpus out to length and unload the lunate facet.
The volar rim is reduced and fixed. For complex injuries, this is usually the keystone on which to build stable fixation.
The dorsal ulnar corner is reduced and fixed if necessary.
Free intra-articular fragments and the dorsal wall fragments are reduced and stabilized as necessary.
Bone graft is applied if the metaphyseal defect is large.
Fixation is completed with a radial column plate.
Depending on the nature of the fracture, fixation may be a subset of these steps.
Approach
The repair is undertaken by means of one of the following approaches:
Limited-incision volar approach (distal limb of Henry approach)
Dorsal approach
Extensile volar approach (FCR approach)
Volar ulnar approach
TECHNIQUES
▪ Limited-Incision Volar Approach
Make a longitudinal incision along the radial side of the radial artery.Related posts:
 Operative Treatment of Finger Carpometacarpal Joint Fracture-Dislocations
Operative Treatment of Finger Carpometacarpal Joint Fracture-Dislocations
 Intramedullary and Dorsal Plate Fixation of Distal Radius Fractures
Intramedullary and Dorsal Plate Fixation of Distal Radius Fractures
 Hemiarthroplasty for Proximal Humerus Fractures
Hemiarthroplasty for Proximal Humerus Fractures
 Open Reduction and Internal Fixation of the Posterior Wall of the Acetabulum
Open Reduction and Internal Fixation of the Posterior Wall of the Acetabulum
 Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures
Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures
 Open Reduction and Internal Fixation of Jones Fractures
Open Reduction and Internal Fixation of Jones Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


