Chapter 2 Fractures: General Management
It is generally accepted that the majority of common fractures can be well managed by the general physician. These injuries are usually easily recognized both clinically and roentgenographically (Fig. 2-1). A satisfactory end result in their treatment will depend not only on the care of the fracture but also on restoration of the function of the injured extremity. These goals are reached by appreciating both the bony and soft tissue structures involved.

Terminology
Fracture: a break in the continuity of a bone
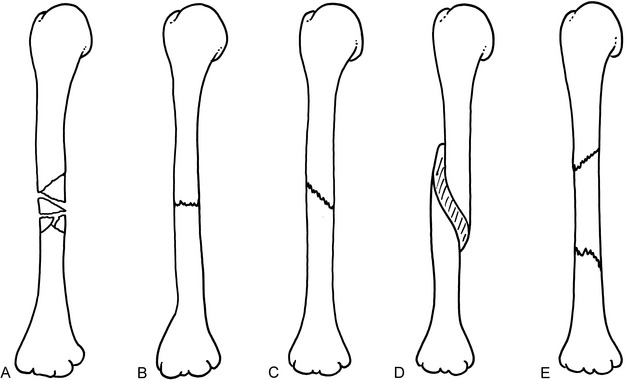
Fig. 2-2 Midshaft fractures of the humerus. A, Comminuted. B, Transverse,undisplaced. C, Oblique, undisplaced. D, Spiral. E, Segmental.
Alignment: rotational or angular position
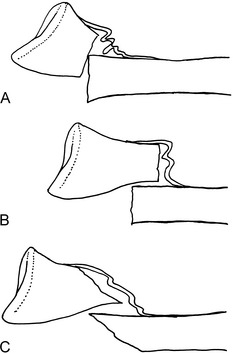
Apposition: amount of end-to-end contact of the fracture (Fig. 2-3)
Fig. 2-3 Apposition and alignment of midshaft fractures of the humerus, anteroposterior (AP) view. A, Perfect end-to-end apposition, perfect alignment. B, Fifty percent end-to-end apposition, perfect alignment. C, Side-to-side (bayonet) apposition, slight shortening, perfect alignment. D, No apposition, approximately 30-degree angulation.
Delayed union: fracture healing that is slower than normal
Dislocation (luxation): disruption in the continuity of a joint
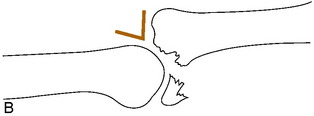
Fracture-dislocation: dislocation that occurs in conjunction with a fracture of the joint. If incomplete, it is called a fracture-subluxation (Fig. 2-4)

Malunion: healing in an unsatisfactory position
Nonunion: failure of bony healing
Pseudarthrosis: failure of bone healing that produces a “false joint” consisting of soft tissue
Subluxation: partial disruption in the continuity of a joint (an incomplete dislocation)
NOTE: Fractures do not dislocate, they displace (shorten, angulate, etc.). They are thus described according to the type, place in the bone, amount of displacement, and angulation (Fig. 2-5). Rotation (torsion) is often difficult to assess roentgenographically but relatively easy to assess clinically. Rotation is usually described in reference to the distal fragment, as is angulation.

General Considerations
INITIAL CARE
A variety of splinting devices are available that make transfer of the patient more comfortable (Fig. 2-6). Their use should be only temporary, however, until the diagnosis is confirmed roentgenographically. These splints should not be kept on more than a few hours, and certainly not overnight. They are very uncomfortable and are not meant for extended use. They fit poorly and do not allow for proper care of the soft tissue and control of swelling.



If definitive treatment of the fracture is to be delayed, a bulky, well-padded soft dressing supplemented with plaster splints, sometimes called the “Robert Jones” dressing, should be applied (Fig. 2-7). This dressing is made by first applying several layers of cast padding or cotton roll circumferentially to the extremity. Plaster splints may then be added, and the entire dressing is secured with gauze or elastic bandage. Precut padded plaster splints should not be used alone without first dressing the limb circumferentially in several layers of cast padding. Remember: the treatment of the soft tissue is as important as the protection of the fracture.

Fig. 2-7 A well-padded bulky dressing reinforced with plaster splints should be applied as soon as possible. Start with many layers of cast padding, because this dressing is temporary and is designed to control swelling and maintain fracture position. After padding is applied, plaster or fiberglass splints are added, and the splints are secured with an elastic bandage or roller gauze. An elastic bandage alone should never be used. It does not immobilize nor “reduce” swelling. It may, in fact, do more harm by further compressing the already compromised lymphatic and venous drainage systems. Short arm splints should be well padded around the wrist. Otherwise, the wrist and hand may “hang” over the edge of the plaster and pain may result.
The extremity is then elevated above the level of the heart, and ice is applied to control swelling. The neurologic and circulatory status of the extremity distal to the injury should always be checked and recorded (Table 2-1). A complete neurologic examination is usually unnecessary. If the patient can extend the thumb and flex and spread the fingers, the major nerves (radial, median, and ulnar) of the upper extremity are functioning; if the patient can flex and extend the toes, the major nerves (posterior tibial and peroneal) to the lower extremity are intact. If a neurologic or vascular impairment is present, it is often relieved by reduction of the fracture or dislocation. If a neurologic impairment persists following the reduction, it is usually treated by simple observation and exercises to prevent contractures. The prognosis is generally good for complete recovery. Circulatory impairment that persists requires immediate vascular evaluation. The initial neurologic examination is particularly important because if a deficit is discovered only after treatment, it may not be able to be determined whether it was present before or occurred as a result of treatment.
Table 2-1 Occasional Neurovascular Complication of Common Injuries
| Bony Injury | Lesion | Prominent Early Findings |
|---|---|---|
| Anterior shoulder dislocation | Circumflex axillary nerve injury | Mid-deltoid numbness |
| Spiral fracture of humerus | Radial nerve injury | Wrist drop |
| Avulsion fracture of medial epicondyle | Ulnar nerve injury | Numbness of small finger, weak finger abduction, adduction |
| Severe elbow fracture | Brachial artery injury | Severe pain, pain on passive finger extension |
| Fractured distal radius, ulna | Median or ulnar nerve injury | Numbness, motor loss |
| Posterior dislocation of hip | Sciatic nerve injury (usually peroneal portion) | Foot drop, weak extensor hallucis longus, numbness on dorsum of foot or great toe |
| Fracture of upper fibula | Peroneal nerve injury | Same |
| Fracture of upper tibia | Compartment syndrome | Severe pain, pain on passive stretch of involved compartment muscles |
Definitive Fracture Care
Some fractures require no treatment or, at most, simple restriction of activity with a sling or crutches (Table 2-2). Many other fractures are treatable by cast immobilization without the need for reduction. Fractures that need to be reduced are usually treated by one of four general methods: (1) open or closed reduction with internal fixation, (2) continuous traction usually followed by cast immobilization, (3) closed reduction with external skeletal fixation, or (4) closed reduction followed by cast immobilization.
Table 2-2 Common Fractures Not Requiring Cast Immobilization*
| Fracture | Treatment |
|---|---|
| Impacted surgical neck of humerus | Shoulder immobilizer |
| Undisplaced radial head fracture | Sling |
| Undisplaced olecranon | Sling |
| Undisplaced patella | Knee immobilizer |
| Shaft of fibula | Crutches |
| Base of fifth metatarsal | Hard sandal |
| Stress fracture | Avoid offending activity |
| Toe phalanges (undisplaced) | Tape to adjacent toe |
| Undisplaced calcaneus | Crutches |
* These fractures are stable and should not displace if the extremity is moved. A soft compression dressing for the first 2 to 3 days may be helpful in some cases.
OPEN OR CLOSED REDUCTION WITH INTERNAL FIXATION
Closed rather than open treatment of most fractures is usually preferred to avoid stripping the soft tissue and periosteum and devascularizing the bone ends. Closed treatment also decreases the chance of infection. There are several fractures, however, in which accurate anatomic positioning of the fragments and rigid internal fixation are beneficial: (1) displaced joint fractures, especially the weight-bearing joints; (2) fractures that cannot be reduced or held by closed methods; (3) fractures of the lower extremity in the elderly to allow early activity; (4) certain epiphyseal fractures that could result in a growth disturbance if not accurately reduced; and (5) joint fractures in which early motion would be helpful to prevent stiffness.
THE ELEMENTS OF CLOSED REDUCTION
Most common fractures can be treated by manual reduction and immobilization, but for this procedure to be successful, certain mechanical aspects of the fracture should be understood. Whenever a bone has been broken and the fractured ends separate, the soft tissue (mainly periosteum) on the side opposite the direction of displacement ruptures and allows the fracture to angulate and rotate (Fig. 2-8). The tissue on the side to which the displacement occurs remains intact, although it may be stripped off of the bone. This intact soft tissue forms a “hinge” that can be used in the treatment of many fractures to help guide the displaced distal fragment or fragments into place and to help maintain that position.

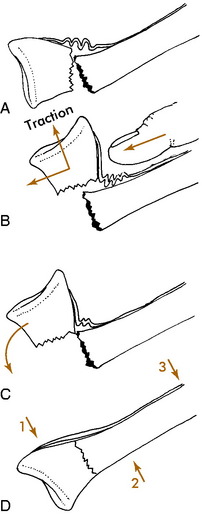
Many methods can be used to place bones back into their original position. Most of these require that the distal fragment be placed into apposition to the proximal one. Some fractures require only a “push” back into place (Fig. 2-9). Others need a more complicated maneuver that incorporates traction and manipulation of the fragments (Fig. 2-10). The nature of the fracture and its displacement determine which method is necessary.