, Paul D. Siney1 and Patricia A. Fleming1
(1)
The John Charnley Research Institute Wrightington Hospital, Wigan, Lancashire, UK
In this clinic, within a period of 2 years and after more than 10 years experience with total hip replacement, the fatigue fracture of the metal of the stem of the femoral prosthesis revealed itself as a definite complication of the operation, and not even an incident of such extreme rarity as hardly to offer a serious problem. (1975)
Charnley’s statement summarizes the effect this complication presented. This, in a way, is not unexpected. The process leading up to the fracture of the stem, or in fact any process especially one spanning a number of years, does not have the same effect as an event. This distinction, between a process and an event, is the essential aspect of the study of long-term results in total hip arthroplasty. In order to chart a process, regular review and recording of information is essential. In joint replacement surgery this demands, not only regular follow-up, but also a collection of detailed and meaningful data which can be used, not merely for research purposes, but more importantly for improvements to be made. Recording the end point, fracture of the stem or a single indication for a revision may be interesting but it fails to provide the vital information concerning the processes leading up to the event – the revision.
Fracture of the original “flat back” Charnley stem in stainless steel, EN58J, was the event that stimulated further research and development of new materials, designs and surgical technique. It may be of interest to recall Charnley’s comment once the initial surprise has passed: “And I thought there was nothing else to do.” So what was the information gathered as the result of a clinical study of the first 17 fractured stems?
Clinical Findings [1]
All, except two fractures occurred in males. The mean age at primary LFA was 60 years (26–82). Their mean weight was 86 kg (57–109). All patients “…had recovered functional capacity equal to that of normal people of the same age.”
In five cases there was a history of trauma “… with the onset of definitive symptoms but almost certainly this … indicated a creeping crack becoming complete.”
Radiological Findings
Position of the stem within the medullary canal was: varus in 9, neutral in 6 and valgus in 2.
Imperfect support (of the stem) by cement presenting as fracture of the cement at the tip of the stem, or separation of the proximal–lateral border of the stem, was observed in seven cases.
The level of the fracture of the stem was between 7 and 10.5 cm from the tip: the segment as risk, measuring 3.5 cm.
Erosion at the level of the medial aspect of the femoral neck, causing defective support of the prosthesis by the cement was considered to be – probably – a universal finding and the cause of fracture of the stem.
At surgery – fragmentation of the cement at the medial femoral neck area was always visible. Whether this was the cause or the effect of the fracture could not be established at surgery. But, taking this finding in conjunction with detailed history, fragmentation of cement must have occurred before stem fracture.
(For a stem to subside within the cement mantle, as with fracture of the cement at the tip of the stem, and to separation from the cement mantle – proximally laterally – proximal medial femoral cement may, at times, fragment. If this cement remains intact and continues to support the stem, the stem will migrate distally with the tip approaching the medial femoral cortex and, therefore, less likely to have moved medially proximally).
The mechanical situation which would favour fatigue fracture of a prosthesis is defective support by the layer of cement which is interposed between the bone of the calcar and the concave upper part of the stem …when this is combined with the firm bonding of the lower part of the stem…
These findings also indicate that distal stem fixation, within the cement, can be near perfect.
Summary
The problem leading to stem fracture was: lack or loss of proximal stem support in the presence of good distal stem fixation. The dimensions of the standard “flat back” stem in EN58J stainless steel were considered inadequate for patients over 77 kg weight [1].
Further Studies of Fracture of the Stem [2]
The review of records of 120 cases of fractures Charnley “flat back” stems has revealed the following information:
The period “at risk” for stem fracture was 11 years from the time of the operation and 97.5 % fractured during that time. Early fractures occurring during the second to fourth year were usually in revisions for a previous stem fracture. If corrosion is a progressive destruction of metal by body fluids, and stainless steel has the fatigue limit characteristic, then the suggestion is that the body environment is non-corrosive. If this interpretation is correct then use of “corrosion resistant” materials does not seem to be justified.
There was a linear relationship between patients’ weight and the time of the fracture.
Radiographic evidence of the failure of full stem fixation was found in 77.2 % of cases where serial radiographs were available.
Loss of proximal stem support, as judged the height of the neck of the femur, was present in 73.3 %.
In patients of comparable weight, stems in valgus position fractured earlier than those in varus position.
Patients of comparable weight, and referred from other units, fractured the stem significantly earlier.
It was considered that the patients’ weight limit for this particular prosthesis should be 66 kg (145 lbs) which was much lower than the 77 kg suggested by Charnley [1].
The Mechanism of Stem Fracture
“Examination of 70 fractured Charnley flat back femoral prostheses, suggested that the causative mechanism was a torsional loading of the proximal portion on the distal part of the stem” [3]
Components collected at revision surgery have always served as “flight recorders”; an invaluable research material. Together with clinical data and good quality radiographs available from regular follow-up, they served as excellent material for modifications and improvements in the design, materials and surgical technique.
Results of the Study
Examination of 70 fractured stems revealed the following information:-
Obliquity of the Fracture (Figs. 22.1 and 22.2)
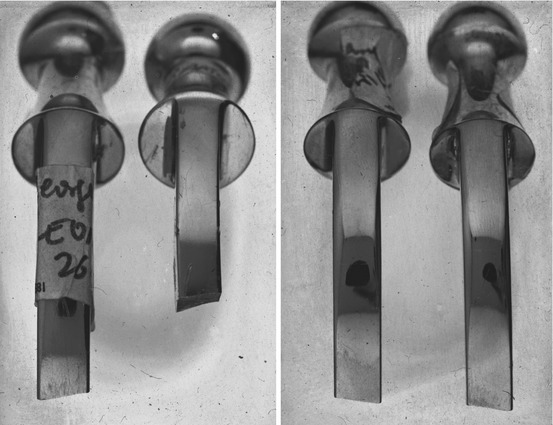
Figs. 22.1 and 22.2
Obliquity of fracture line, viewed from the lateral aspect, identifies the site – left or right (Reproduced from Wroblewski [9])
Viewed from the lateral aspect the fracture line was always at an angle to the long axis of the stem. From the direction of the obliquity it was possible to determine the side from which the specimen was retrieved; the obliquity was always upwards away from the operated side. The degree of the slope varied from 2 to 20° with an average of 9.9°. The degree of the slope of the fracture was considered to reflect and be proportional to, the length of the stride, assuming of course that the stem remained positioned in the coronal plane.
Related posts:
 Arthroplasty of the Hip: A New Operation
Arthroplasty of the Hip: A New Operation
 Results of Low-Friction Arthroplasty of the Hip Performed as a Primary Intervention
Results of Low-Friction Arthroplasty of the Hip Performed as a Primary Intervention
 Revision for Recurrent or Irreducible Dislocation
Revision for Recurrent or Irreducible Dislocation
 Increasing Follow-Up: Changing Age Patterns
Increasing Follow-Up: Changing Age Patterns
 Bone-Cement Interface: The Cup: Radiographic Appearances
Bone-Cement Interface: The Cup: Radiographic Appearances
 Factors Affecting Wear of the UHMWPE Cup
Factors Affecting Wear of the UHMWPE Cup
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


