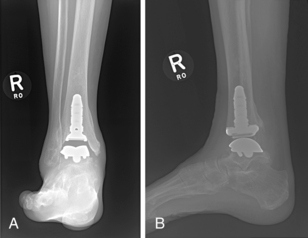
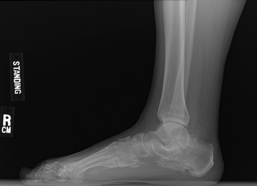
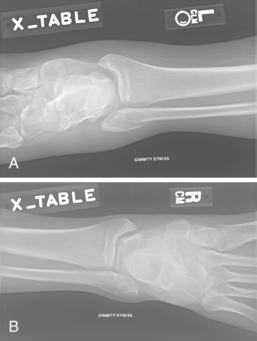
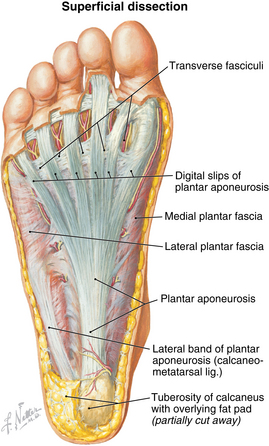
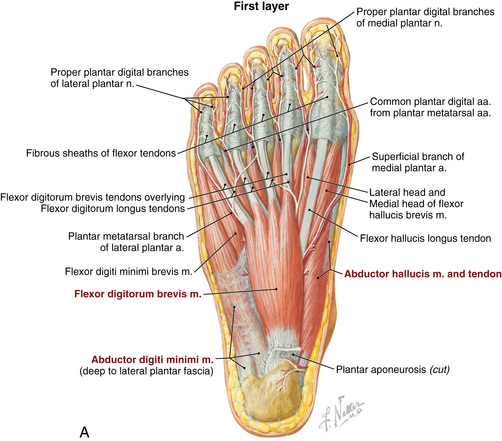
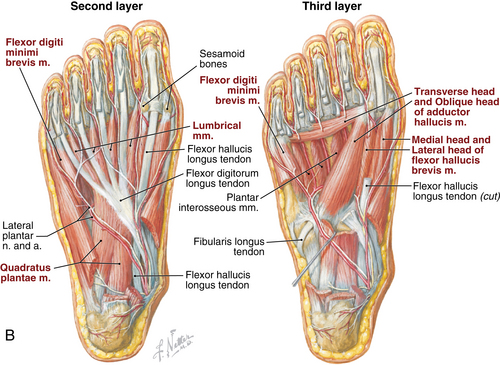
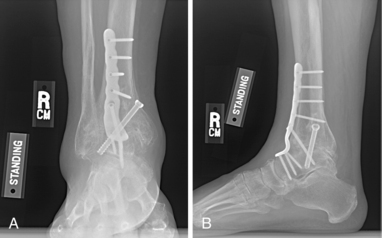
8 Foot and ankle Figure 8-3. Dorsal view of the foot sole. (From Netter illustration from www.netterimages.com. Copyright Elsevier Inc. All rights reserved.) Figure 8-4A-B. Plantar views of the foot muscles. (From Netter illustration from www.netterimages.com. Copyright Elsevier Inc. All rights reserved.) Table 8-2. Normal Ankle/Foot Range of Motion Table 8-4. • Generally has limited value and indicated only in mild arthritis without significant joint space narrowing • Indications: painful tibiotalar arthritis not responsive to nonoperative treatment, failed arthroplasty • Contraindications: acute infection, acute neuropathic arthropathy, severe vascular disease • Indications: tibiotalar arthritis not responsive to nonoperative management, low demand patients older than age 50-55 years, weight < 200 lb, maintained range of motion, normal/near normal alignment, no preexisting subtalar arthritis. • Contraindications: acute infection, significantly diminished bone stock, neuropathy, severe vascular disease. Relative contraindications include deformity greater than 5 degrees and talar avascular necrosis. • Major risks include nonunion (<10%), wound complications, nerve injury, infection, deep vein thrombosis (DVT), hardware loosening/failure, and development of arthritis in hindfoot/subtalar joint. A risk of amputation exists in cases of severe complication (≤5%). • The complication rate increases with nicotine use, neuropathy, and vascular disease. • Informed consent and counseling: Risks are similar to arthrodesis (infection, wound complications, DVT, hardware loosening). Recent studies report 10% to 30% reoperation rate and survival rates of 77% to 90% at 5- and 10-year follow-up. If surgery fails, consider conversion to arthrodesis (contraindicated in infection). Limited revision options are available. Figure 8-8. Postoperative anteroposterior (A) and lateral (B) views following ankle arthrodesis using anterior plate. • Many implants for fixation are available, the most common being an anterior plate with cross-screws. An intraoperative radiograph is used to confirm appropriate placement. • Open anterior approach is most common. An incision is made over the ankle between anterior tibial tendon and extensor hallucis longus (EHL). • Structures at risk include superficial peroneal nerve and neurovascular bundle (posterior to EHL). • The neurovascular bundle is mobilized, and the tibial osteophytes are removed to visualize joint. The joint is prepared by removing any remaining articular cartilage, and microfracturing and/or drilling the subchondral bone. A lamina spreader can be helpful for visualization. • Align neutral dorsiflexion/plantarflexion, 0 to 5 degrees hindfoot valgus, 5 degrees external rotation. An intraoperative radiograph is used to determine correct alignment for fixation. • A sugar tong splint is applied in the operating room after closure. The patient remains non–weight bearing. • Sutures are removed and radiographs are obtained. A non–weight-bearing cast is applied for 4 weeks. • Radiographs reviewed. The patient is transitioned to a weight-bearing cast for an additional 6 weeks. • Remove cast. Obtain radiographs to evaluate for healing. • Physical therapy is generally not indicated, but some patients may need some therapy for gait training. • Second- and third-generation implants are now available, but there are still limited data on longevity. First-generation implants have a high failure rate. • Both 2 and 3 component implants are available, primarily depending on surgeon preference. • An open anterior approach is used as described in ankle arthrodesis. Major structures at risk include the superficial peroneal nerve and neurovascular bundle. Initial treatment should be nonoperative. NSAIDs, lace-up ankle brace, weight loss if indicated, activity modification (limit uneven surfaces), and corticosteroid injections • Lateral incision is made about 2 cm distal to lateral malleolus, extending to the base fourth metatarsal. Extensor digitorum brevis is reflected to expose subtalar joint. Peroneal tendons are elevated from lateral calcaneous and retracted. • Any remaining cartilage is removed, and the joint is debrided to cancellous bone. • Fusion is performed at 5 degrees valgus. Two cannulated screws are placed from the non–weight-bearing portion of calcaneus toward the anterior margin posterior facet into the talus. Divergent screws have improved compression forces compared with parallel screws or a single screw. Intraoperative radiographs and guidewires are used to ensure appropriate placement of screws (Fig. 8-11). Figure 8-11. Lateral radiograph status post subtalar arthrodesis using two divergent cannulated screws. • The patient may require bone grafting or bone block if bone loss is present from previous trauma/calcaneal fracture. • A posterior splint is applied in the operating room after closure. The patient remains non–weight bearing for 2 weeks. • Weight-bearing ankle AP, mortise, lateral. Assess fracture, alignment, displacement. • Weight bearing foot AP, oblique, lateral. Assess for fracture or malalignment. • Stress radiographs of the ankle should be performed for isolated fibular fractures at the level of the ankle joint. To perform, gravity stress or external rotation and/or abduction stress is applied in a non–weight-bearing mortise view. Medial clear space greater than 4 to 5 mm indicates deltoid ligament injury and ankle instability (Fig. 8-12). • Compare with contralateral ankle (mortise view is best). A 2-mm side-to-side difference in medial clear space indicates instability. • CT scans are helpful to evaluate comminution and subtle displacement. Scan should be performed of bilateral ankles to compare syndesmosis and medial clear space. • MRIs are usually not necessary but can be useful to evaluate the deltoid ligament and help determine ankle stability. • Type A: Transverse fracture at the level of or distal to the tibial plafond • Type B: Spiral, oblique fracture at the level of distal tibiofibular joint and extends proximally. Associated with possible disruption of syndesmosis (Fig. 8-13). • Type C: Fracture proximal to distal tibiofibular joint. Syndesmosis completely disrupted; anterior and posterior tibiofibular ligaments and interosseous membrane ruptured (Fig. 8-14) • Immobilization in cast or walking boot, weight bearing as tolerated. Most fractures heal in 6 weeks. • Consider nonoperative management when medial clear space is less than 4 to 5 mm and less than 2 mm greater than contralateral side on stress and static radiographs. • Immobilization in cast or walking boot for 6 weeks. Weight bearing is progressed as tolerated. • Frequent follow-up with radiographs (weekly for first 2 to 3 weeks). Surgical fixation is recommended if there is a change in stability or alignment. • After 6 weeks of immobilization, transition to brace. Physical therapy may be helpful to regain motion and strength. • Distal fibular fractures—Multiple hardware options are available including locking and nonlocking plates and screws. Locking plates should be used when bone quality is poor or a patient is at high risk for nonunion (diabetes, osteoporosis). • Medial malleolus fractures—Fixation devices include lag, partially threaded, or cannulated screws; Kirshner wires; tension bands; and buttress plate (used only for vertical sheer fractures to prevent proximal migration of fracture fragment). • Dorsal approach: A longitudinal incision is made over the involved web space. The dorsal interosseous fascia is split and retracted. Interosseous muscle is partially detached, metatarsal heads are retracted, and the intermetatarsal ligament is cut. The neuroma is exposed by retracting the digital artery and lumbrical muscle. • Plantar approach: This is generally reserved for revision procedures. A longitudinal incision is made between the metatarsal heads. The plantar fascia is split and retracted to expose the neuroma. • Once neuroma is exposed, it is dissected proximally and cut. The proximal stump retracts into the intrinsic muscles. • Evaluate vascular status after excision to ensure digital artery intact and functioning. • Inspect for presence of corns or calluses, open wounds, swelling, trophic changes, dependent rubor (arterial insufficiency), and bony prominences. • Ulcers often develop at sites of callus formation or as a result of microtrauma. • Increased warmth compared with the contralateral side can indicate Charcot arthropathy, venous insufficiency, or infection. • May be normal in early disease processes • Difficult to differentiate Charcot arthropathy from osteomyelitis • Charcot arthropathy: disorganization of bony structure, bony erosion, intra-articular loose bodies, may have subluxation or dislocation of joints (Fig. 8-16) • Risk Category 0: Normal appearance and sensation, mild to no deformity • Risk Category 1: Normal appearance, insensate, no deformity • Risk Category 2: Insensate foot with deformity, no history of prior ulcer • Risk Category 3: Insensate foot with deformity and history of prior ulcer • Stage 0: Clinical examination findings of erythema and edema. Radiographs are normal. • Stage I: Fragmentation or dissolution phase. Radiographs demonstrate periarticular fragmentation, subluxation, or dislocation of joint. On examination, foot is warm, edematous, and erythematous. • Stage II: Coalescence period, early healing phase. Radiographs show early sclerosis, fusion of bony fragments, and absorption of debris. On examination, there is less erythema and warmth than stage I. • Stage III: Reconstruction phase. Radiographs reveal subchondral sclerosis, osteophytes, and narrow or absent joint spaces. On examination, visual deformity is present and there is no acute inflammation. • Risk Category 0: education, normal footwear, yearly clinical examination • Risk Category 1: education, daily foot self-examination, protective over-the-counter insoles, appropriate footwear, biannual clinical examination • Risk Category 2: education, daily foot self-examination, custom pressure-dissipating accommodative orthoses, inlay depth soft-leather shoes, clinical examination every 4 months • Risk Category 3: education, daily foot self-examination, custom pressure-dissipating orthoses, inlay depth soft-leather shoes, clinical examination every 2 months • Stage I: immobilization using total contact casting, which reduces total load on the foot by one third. Length of immobilization depends on progression of disease/collapse, often 2 to 4 months. • Stage II: ankle-foot orthosis or Charcot restraint orthotic walker (CROW) boot. • Stage III: accommodative shoe and custom insole to decrease pressure on bony prominences • Procedure: Longitudinal incision is made at the border of plantar and dorsal skin. Careful dissection to prominent exostosis and prominent bone is excised using an osteotome or saw. Edges of bone are then smoothed, and precise closure is completed. • Zone 1 (avulsion): Fifth metatarsal tuberosity fracture. Most common type (>90%). Often extends from insertion of peroneal brevis to involve the tarsometarsal joint. • Zone 2 (Jones fracture): Distal to the tuberosity at metaphyseal-diaphyseal junction. Fracture extends to fourth to fifth intermetatarsal joint. Mechanism is adduction or inversion of the forefoot (Fig. 8-18). • Zone 3: Proximal diaphyseal shaft fracture. Rare, less than 3% of fifth MT fractures. Frequently a stress injury and patients may report prodromal pain.
Anatomy
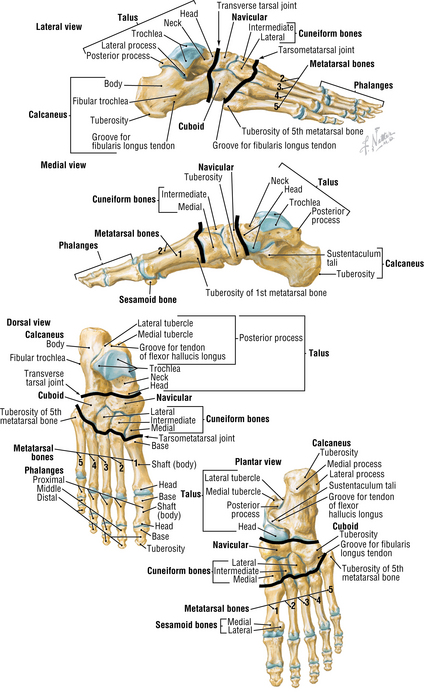
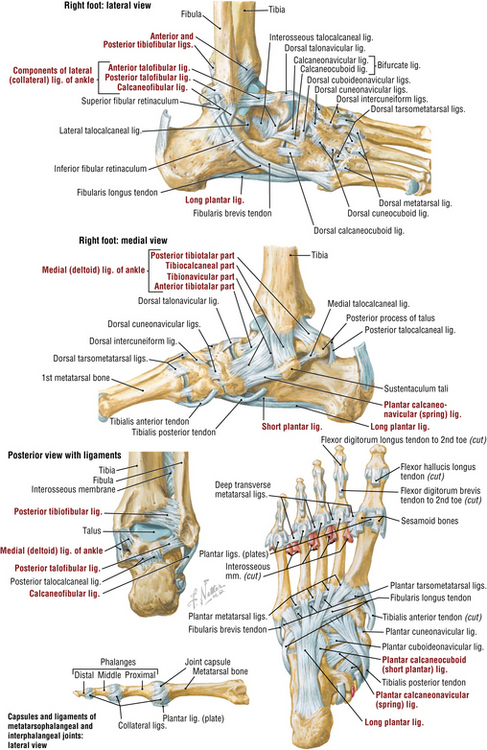
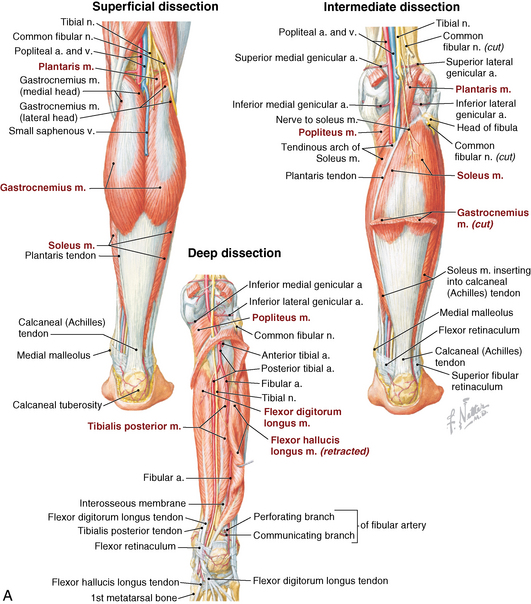
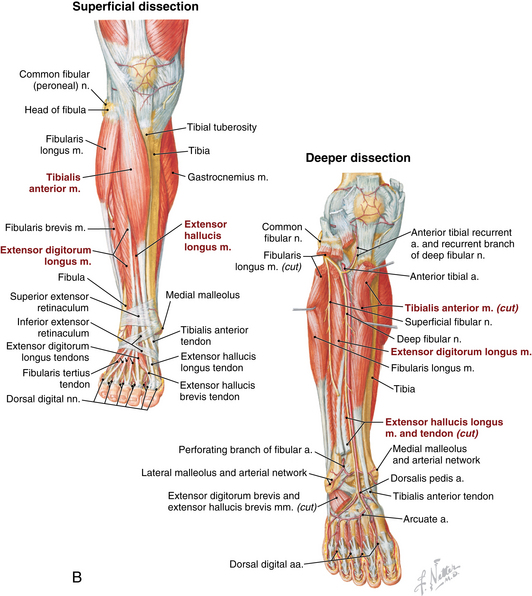
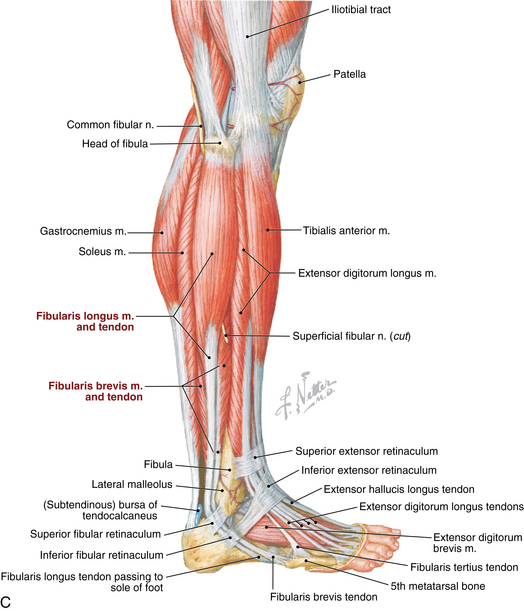
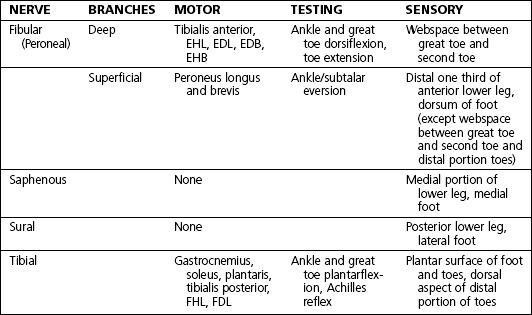
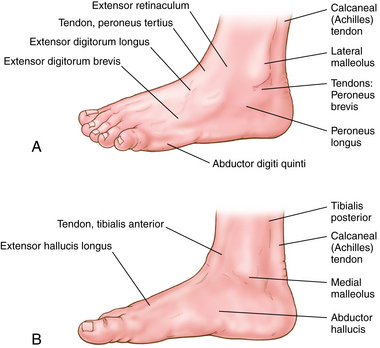
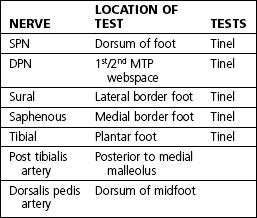
Muscles, nerves, arteries: Figures 8-3, 8-4AB, and 8-5A-C
Physical examination
 Inspect for edema, erythema, ecchymosis, deformity, callus formation, ulceration, and hairlessness. On standing examination, note hindfoot alignment. Assess gait pattern.
Inspect for edema, erythema, ecchymosis, deformity, callus formation, ulceration, and hairlessness. On standing examination, note hindfoot alignment. Assess gait pattern.
 Palpate to evaluate clinical complaint:
Palpate to evaluate clinical complaint:
Normal range of motion: Table 8-2
Ankle dorsiflexion
10-23 degrees
Ankle plantarflexion
23-48 degrees
Inversion
5-35 degrees
Eversion
5-25 degrees
First metatarsophalangeal dorsiflexion
45-90 degrees
First metatarsophalangeal plantarflexion
10-40 degrees
Differential diagnosis: Table 8-4
Anterior ankle pain
Ankle arthritis, osteochondral dessicans talus
Medial ankle pain
Posterior tibial tendinopathy, medial malleolar injury
Lateral ankle pain
Peroneal tendinopathy, ankle sprain
Posterior ankle pain
Achilles tendinopathy or rupture, os trigonum, posterior impingement
Midfoot
Lisfranc injury, midfoot arthritis
Forefoot
Metatarsal fracture, stress fracture, metatarsalgia
Heel pain
Plantar fasciitis, calcaneal stress fracture, insertional Achilles tendinopathy
Great toe
Hallux rigidus, hallux valgus
Lesser toes
Toe fracture, hammertoe deformity, Morton neuroma
Ankle arthritis
Imaging
 Radiographs: Weight-bearing anteroposterior (AP), mortise, lateral
Radiographs: Weight-bearing anteroposterior (AP), mortise, lateral
Treatment options
Operative management
Operative indications
 Ankle arthrotomy with debridement/loose body removal
Ankle arthrotomy with debridement/loose body removal
Informed consent and counseling
Surgical procedures
 Ankle arthrodesis (Fig. 8-8AB)
Ankle arthrodesis (Fig. 8-8AB)
Estimated postoperative course
 Total ankle arthroplasty (Fig. 8-9AB)
Total ankle arthroplasty (Fig. 8-9AB)
Subtalar arthritis
Imaging
Treatment options
Operative management
Operative indications
Informed consent and counseling
 Risks include infection, wound complications, arthritis in surrounding joints, nonunion (reported rates 0.5%), DVT, symptomatic hardware (especially if screw heads are prominent posteriorly). Some patients feel instability on uneven ground. At-risk structures: superficial peroneal and sural nerves, peroneal tendons
Risks include infection, wound complications, arthritis in surrounding joints, nonunion (reported rates 0.5%), DVT, symptomatic hardware (especially if screw heads are prominent posteriorly). Some patients feel instability on uneven ground. At-risk structures: superficial peroneal and sural nerves, peroneal tendons
Surgical procedure

Estimated postoperative course
 Postoperative 2 weeks: sutures removed. Non–weight bearing in a boot. Remove boot multiple times daily for ankle motion to prevent stiffness.
Postoperative 2 weeks: sutures removed. Non–weight bearing in a boot. Remove boot multiple times daily for ankle motion to prevent stiffness.
 Postoperative 6 weeks: radiograph reviewed. Start weight bearing in boot from weeks 6 to 12.
Postoperative 6 weeks: radiograph reviewed. Start weight bearing in boot from weeks 6 to 12.
Ankle fractures
Physical examination
 Edema, ecchymosis, tenderness over fracture site. Medial tenderness without medial malleolus fracture suggests deltoid ligament injury; does not necessarily signify unstable ankle joint
Edema, ecchymosis, tenderness over fracture site. Medial tenderness without medial malleolus fracture suggests deltoid ligament injury; does not necessarily signify unstable ankle joint
 Fracture blisters with severe edema and soft tissue trauma
Fracture blisters with severe edema and soft tissue trauma
 Visual deformity present if ankle dislocated or severe displacement of fracture
Visual deformity present if ankle dislocated or severe displacement of fracture
Imaging
Classification systems
 Danis-Weber classification is based on the location of the fibular fracture and does not address the medial structures.
Danis-Weber classification is based on the location of the fibular fracture and does not address the medial structures.
Initial treatment
 Immobilization in sugar tong splint, non–weight bearing, and elevation. Refer to an orthopaedic surgeon to be seen within 7 to 10 days.
Immobilization in sugar tong splint, non–weight bearing, and elevation. Refer to an orthopaedic surgeon to be seen within 7 to 10 days.
Treatment options
 Weber A fractures: Nearly all can be treated nonoperatively, even with mild displacement.
Weber A fractures: Nearly all can be treated nonoperatively, even with mild displacement.
 Weber C: Nonoperative management is not recommended.
Weber C: Nonoperative management is not recommended.
Operative management
Codes
Informed consent and counseling
 Risks include wound complications, infection, nonunion, and DVT. The rate of complication is significantly higher in diabetics, nicotine users, and patients with peripheral vascular disease. Post-traumatic arthritis may still occur despite proper stabilization. Major structures at risk are the superficial peroneal nerve (crosses fibula approximately 4 to 5 cm proximal to joint) and saphenous vein (for medial incisions).
Risks include wound complications, infection, nonunion, and DVT. The rate of complication is significantly higher in diabetics, nicotine users, and patients with peripheral vascular disease. Post-traumatic arthritis may still occur despite proper stabilization. Major structures at risk are the superficial peroneal nerve (crosses fibula approximately 4 to 5 cm proximal to joint) and saphenous vein (for medial incisions).
Surgical procedure
 Open Reduction, Internal Fixation
Open Reduction, Internal Fixation
 Use a lateral approach for fixation of distal fibula, syndesmosis, and possibly posterior malleolus. Longitudinal incision is made directly over the distal fibula. Fibular fracture is reduced and stabilized, restoring proper length and rotation. Intraoperative radiograph is used for reduction, to confirm proper screw length, and to determine stability. After ORIF fibula, a radiograph is taken to evaluate medial clear space. If widening is present after ORIF fibula, a syndesmotic screw is placed (Fig. 8-15).
Use a lateral approach for fixation of distal fibula, syndesmosis, and possibly posterior malleolus. Longitudinal incision is made directly over the distal fibula. Fibular fracture is reduced and stabilized, restoring proper length and rotation. Intraoperative radiograph is used for reduction, to confirm proper screw length, and to determine stability. After ORIF fibula, a radiograph is taken to evaluate medial clear space. If widening is present after ORIF fibula, a syndesmotic screw is placed (Fig. 8-15).
 Many fractures require both medial and lateral approaches.
Many fractures require both medial and lateral approaches.
Estimated postoperative course
 Postoperative 2 to 3 weeks: Sutures removed. Radiographs are obtained at each postoperative visit until complete healing is noted.
Postoperative 2 to 3 weeks: Sutures removed. Radiographs are obtained at each postoperative visit until complete healing is noted.
 Postoperative 8 to 10 weeks: Discontinue boot and progress to shoe with ankle brace.
Postoperative 8 to 10 weeks: Discontinue boot and progress to shoe with ankle brace.
Plantar fasciitis (PF)
Morton’s (intermetatarsal) neuroma
Physical examination
 Tenderness to palpation of intermetatarsal space. Pain is not reproduced with palpation of metatarsal heads or metatarsal-phalangeal (MTP) joints.
Tenderness to palpation of intermetatarsal space. Pain is not reproduced with palpation of metatarsal heads or metatarsal-phalangeal (MTP) joints.
 Mulder’s sign: Squeeze forefoot medial to lateral and apply dorsal pressure over affected web space. Positive test is audible or palpable click that causes pain.
Mulder’s sign: Squeeze forefoot medial to lateral and apply dorsal pressure over affected web space. Positive test is audible or palpable click that causes pain.
Imaging
Treatment options
Surgical procedure
Estimated postoperative course
 Dorsal approach: weight bearing as tolerated in hard-soled post-operative shoe. Progress to normal shoe wear and activities as tolerated once incision healed, usually between 2 and 3 weeks postoperative.
Dorsal approach: weight bearing as tolerated in hard-soled post-operative shoe. Progress to normal shoe wear and activities as tolerated once incision healed, usually between 2 and 3 weeks postoperative.
 The plantar approach requires greater protection with a splint or cast boot and more limited weight bearing to prevent wound complications. Sutures are removed 2 to 3 weeks postoperative. Progress to normal shoe wear and activities as tolerated once the wound has completely healed. This may be 3 to 4 weeks postoperative.
The plantar approach requires greater protection with a splint or cast boot and more limited weight bearing to prevent wound complications. Sutures are removed 2 to 3 weeks postoperative. Progress to normal shoe wear and activities as tolerated once the wound has completely healed. This may be 3 to 4 weeks postoperative.
Diabetic foot and charcot arthropathy
Physical examination
 Visual deformities: Claw-toe deformities are common from loss of intrinsic muscle tone. Rocker-bottom midfoot deformity is often present in Charcot arthropathy of midfoot.
Visual deformities: Claw-toe deformities are common from loss of intrinsic muscle tone. Rocker-bottom midfoot deformity is often present in Charcot arthropathy of midfoot.
Imaging
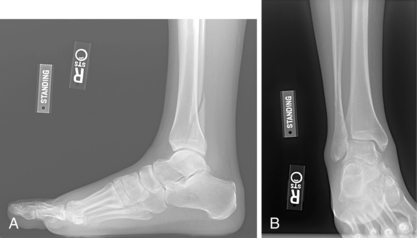
 Radiograph: weight-bearing AP, lateral, oblique of foot and AP, lateral, mortise of ankle
Radiograph: weight-bearing AP, lateral, oblique of foot and AP, lateral, mortise of ankle
Classification systems
 Multiple classification systems for diabetic foot ulcers, and Charcot arthropathy
Multiple classification systems for diabetic foot ulcers, and Charcot arthropathy
 Pinzer “risk factor” system to guide treatment of diabetic patients
Pinzer “risk factor” system to guide treatment of diabetic patients
 Classification system of Charcot arthropathy:
Classification system of Charcot arthropathy:
Treatment options
 At-risk patients without Charcot arthropathy: based on Pinzur classification
At-risk patients without Charcot arthropathy: based on Pinzur classification
 Charcot arthropathy: based on stage
Charcot arthropathy: based on stage
Surgical procedures
 Amputation: Level of amputation and surgical techniques vary, depending on disease involvement.
Amputation: Level of amputation and surgical techniques vary, depending on disease involvement.
 Arthrodesis: As described in earlier sections of the chapter
Arthrodesis: As described in earlier sections of the chapter
Exostectomy
 Estimated postoperative course
Estimated postoperative course
Metatarsal fractures (including jones fracture)
Imaging
Classification system
 Fifth metatarsal fractures are classified on the basis of location. Treatment recommendations are based on this classification system.
Fifth metatarsal fractures are classified on the basis of location. Treatment recommendations are based on this classification system.