(1)
Department of Orthopedic Surgery Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Abstract
Because of the close relation of the flexor hallucis longus tendon and os trigonum, tendinitis of the flexor hallucis longus is often present in patients with a posterior impingement of the ankle. Isolated tendinitis of the flexor hallucis longus does exist. Release of the flexor hallucis longus by means of a two-portal hindfoot approach compares favorable to open surgery. The etiology, history, physical examination, and treatment options and operative technique are described in this chapter.
A patient with flexor hallucis longus tendinitis has pain behind the medial malleolus on forced movements of the big toe.
Posterior ankle impingement is often combined with flexor hallucis longus tendinitis
Release of the flexor hallucis longus by means of a 2-portal hindfoot approach compares favorable to open surgery.
15.1 Introduction
Posteromedial overuse and posttraumatic injuries in sports like ballet dancing and soccer can be caused by an isolated tenosynovitis of the flexor hallucis longus tendon or a flexor hallucis longus tendonitis combined with a posterior impingement syndrome (Van Dijk and Van Bergen 2008). Because of the close relation of the flexor hallucis longus to the posterior talar process often a combination of tendonitis and posterior impingement of the ankle co-exist. We reported on 58 consecutive patients with posterior ankle impingement. In this group 63 % of the patients experienced symptomatic involvement of the flexor hallucis longus tendon (Scholten et al. 2008). The associated tenosynovitis of the flexor hallucis longus can be explained by a slight displacement of an os trigonum, by reactive synovitis, capsular hypertrophy or scar tissue in the posterior ankle area (De Leeuw and Van Dijk 2009).
15.2 Etiology
Medial from the posterior talar process the flexor hallucis longus runs in a sliding channel. This sliding channel is located in between the posterior talar process and the posteromedial talar process (Figs. 15.1 and 15.2). At this level the tendon is enclosed by a flexor retinaculum. In case of hypertrophy of the muscle belly this thickened part of the musculotendinious portion is pulled into this narrow channel. This is especially the case when the ankle and big toe are both simultaneous in a hyperdorsiflexed position. In ballet dancers typically the grand plié position (= maximum dorsiflexion of the ankle joint and big toe at the same time) pulls the muscle belly into the sliding channel. This can lead to local tenosynovitis and thickening of the tendon (Fig. 15.3). Another mechanism involves this slight displacement of an os trigonum in case of posterior impingement. In exceptional cases we find a double flexor hallucis longus tendon running in the same gliding channel (Fig. 15.4a, b) or in a separate tunnel (Fig. 15.5).
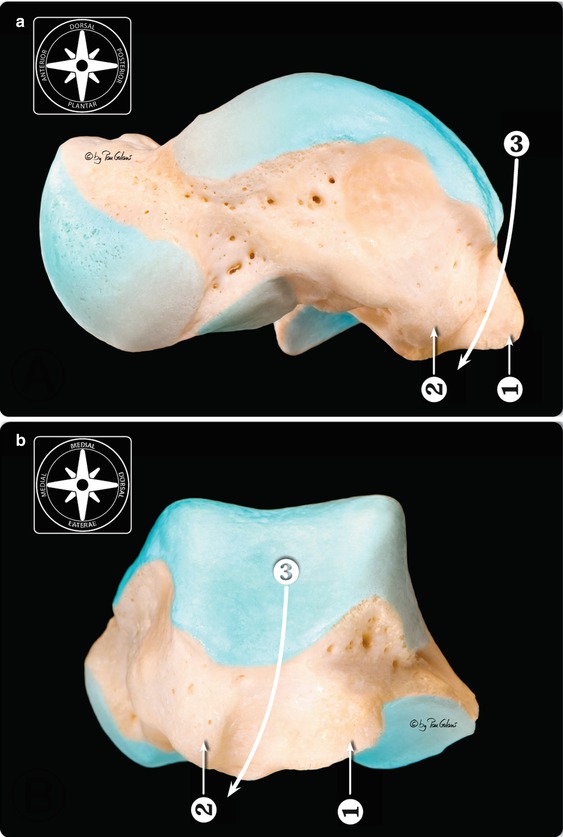
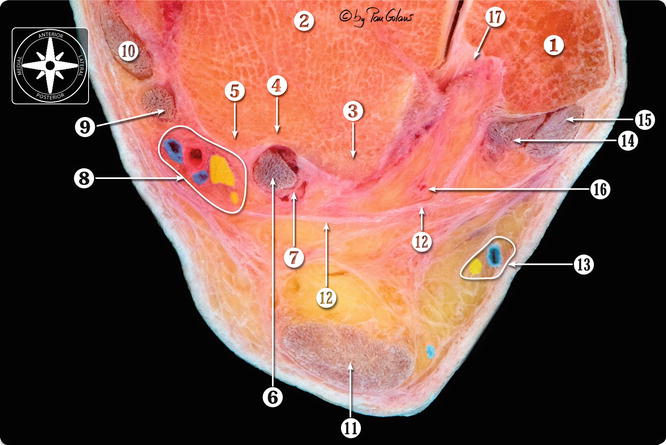
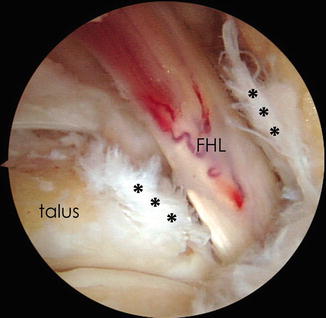
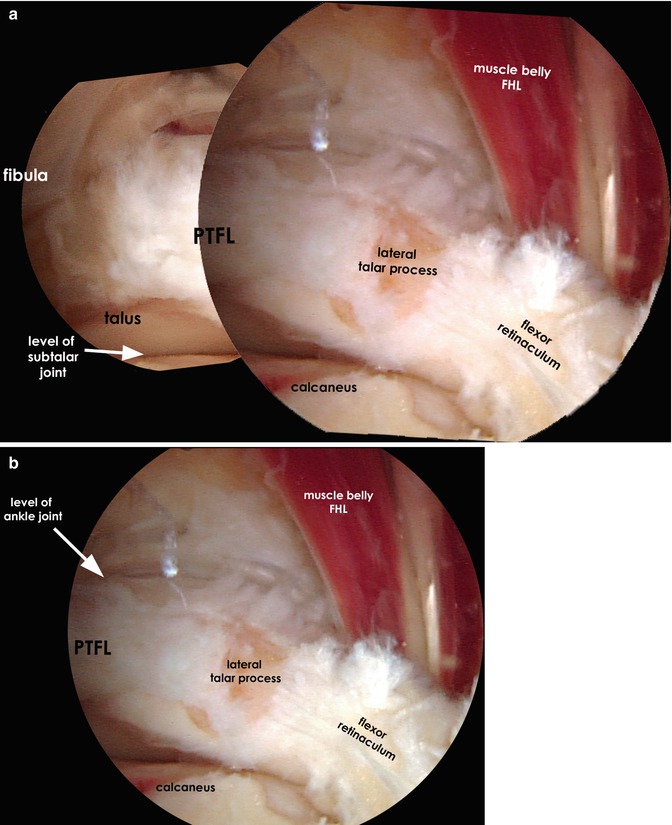
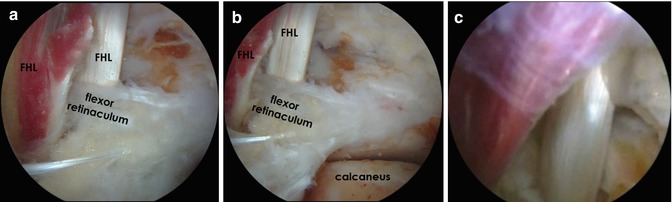
Fig. 15.1
(a) Medial view of the right os talus. (b) Posterior view of the right os talus. 1 Lateral talar process. 2 Medial talar process. 3 Flexor hallucis longus tendon traject. The articular surfaces have been colored by photo editing software (With kind permission of © Pau Golanó 2013)
Fig. 15.2
Transversal section of the ankle joint at the level of the talar process. Posterior detail. 1 Lateral malleolus. 2 Body of the talus. 3 Lateral talar process. 4 Flexor hallucis longus tendon groove 5 Medial talar process. 6 Flexor hallucis longus tendon. 7 Flexor hallucis longus retinaculum. 8 Posterior neurovascular bundle (Tibial nerve and posterior tibial artery and veins). 9 Flexor digitorum longus tendon. 10 Tibialis posterior tendon. 11 Calcaneal or Achilles tendon. 12 Deep crural fascia or fibulotalocalcaneal ligament (Rouvière and Canela ligament). 13 Sural nerve and small saphenous vein. 14 Peroneus brevis tendon. 15 Peroneus longus tendon. 16 Posterior peroneal artery. 17 Malleolar groove and insertion of the posterior talofibular ligament, transverse ligament and posterior intermalleolar ligament (With kind permission of © Pau Golanó 2013)
Fig. 15.3
Left ankle. Posterior view (arthroscope in the posterolateral portal). The flexor retinaculum has been cut. We see the remnants of the flexor retinaculum medial and lateral from the FHL (asterisks). The neovascularisation on the flexor tendon as a sign of chronic irritation and repair is clearly visible
Fig. 15.4
(a) Patient with chronic posteromedial ankle pain. Clinically FHL tendinopathy with recognizable tenderness on palpation on the flexor hallucis longus behind the medial malleolus. Apart from the FHL tendinopathy the patient had a posteromedial impingement with recognizable tenderness on the hyperplantar flexion test. The X-ray showed a prominent posterior talar process (no os trigonum). It was decided to release the FHL and reduce the posterior talar process. (3A) Arthroscopic view from posterior. It is the left ankle and the scope is in the posterolateral portal. We see the subtalar joint as well as the ankle joint. In the middle of the view we see the lateral posterior talar process and attached to it on the lateral side the posterior talofibular ligament (PTFL) and on the medial side the flexor retinaculum. We see two separate FHL tendons with muscular fibres running very deep down. This double FHL is an anatomic variation. Normally the muscle belly does not reach to the level of the flexor retinaculum. (b) Closer look of the same patient as in (a). The double flexor hallucis tendon with muscle belly is clearly visible. Treatment consists of release of the flexor retinaculum and reduction of the posterior talar process. The patient became symptom free
Fig. 15.5




Patient with posterior ankle pain with positive posterior impingement test. X-ray did not show a hypertrophic posterior talar process and no os trigonum. Clinically there was no FHL tendinopathy. Patient underwent posterior arthroscopy under the diagnosis of posterior soft tissue impingement. During arthroscopy a double FHL tendon was found with low riding muscle belly of the most posterior FHL tendon. The two FHL tendons were located in separate channels, divided by a flexor retinaculum. Treatment consisted of removal of the soft tissue impediment. No further release of the FHL was performed. The posterior ankle pain diminished significantly after the operation. The patient was satisfied with the outcome and could resume her sporting activities. (a) Posterior view right ankle. Scope is in the posterolateral portal. We see the FHL tendon in the middle of the picture and behind it we see a second flexor hallucis longus tendon with a low riding muscle belly. In between both tendons we see a flexor retinaculum and posterior from the posterior FHL tendon we see a second retinaculum. (b) In this picture we see the two FHL tendons in relation to the posterior talar process, the double flexor retinaculum and the subtalar joint. (c) View more proximal showing the large muscle belly of the most posterior FHL muscle tendon unit
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
