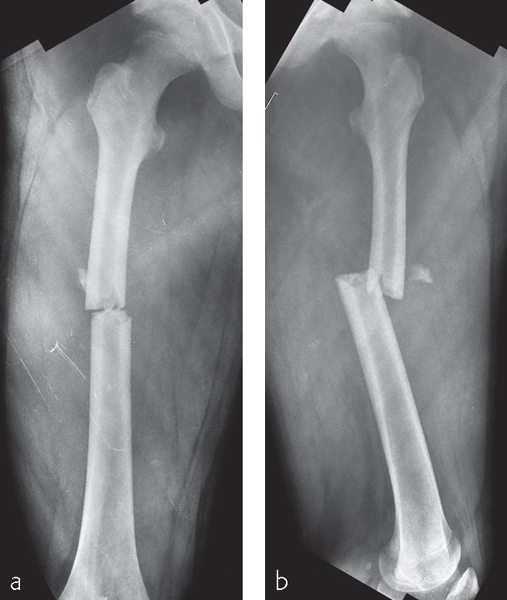
Femur, shaft: simple fracture, transverse
Case description
A 13-year-old boy sustained a closed, transverse fracture of the right femoral shaft after being hit by a car. He was over-weight for his age.
Indication for MIPO
Pediatric femoral shaft fractures can be treated with different methods depending on the age and weight of the patient. The TEN is an ideal option for pediatric femoral shaft fractures in young children, but it was not suitable in this case, since the patient was over 10 years old and overweight for his age. Rigid intramedullary nailing may be considered, but it can destroy the blood supply to the femoral head resulting in avascular necrosis. The length and intramedullary canal of the femur is small for the standard size of the nail, In this case, plating is the recommended alternative. When plating is used, MIPO should be considered as this technique preserves blood supply to the fracture fragments.
Preoperative planning
A good preoperative plan helps to facilitate the subsequent execution of the surgical procedure. The plan should include the surgical approach, a graphic representation of the fracture fragments, the reduction technique, the most appropriate implant, and the sequential steps required in its application ( Fig 23.4-2 ).

Operating room setup
Anesthesia
General anesthesia is usually recommended for children.
Patient and image intensifier positioning
The patient is positioned supine on a radiolucent operating table. Placing a pad under the patient‘s ipsilateral buttock prevents the leg from externally rotating so the surgeon does not need to hold the leg during the procedure ( Fig 23.4-3 ). Preparing and draping both lower extremities in patients with complex fractures will allow for better assessment of leg length, alignment, and rotation by comparison with the uninjured leg. Improved lateral proximal view with image intensification is accomplished by elevating the opposite leg. The C-arm is positioned on the opposite side of the injured leg. A preoperative image of the contralateral hip and knee using image intensification can be helpful to check correct mechanical axis of the femur.
Related posts:
 Clavicle—introduction
Partially unstable pelvic ring injury: bilateral anterior pubic root fractures and a disruption of the left sacroiliac joint—61-B2.2
Pelvis, acetabulum: both-column acetabular fracture—62-C2 and 62-C7 body fracture
Femur, proximal: extraarticular fracture, intertrochanteric—31-A3 and wedge diaphyseal fracture—32-B1
Tibia and fibula, proximal: intraarticular bicondylar fracture, no metadiaphyseal involvement—41-C3
Tibia and fibula, shaft—introduction
Clavicle—introduction
Partially unstable pelvic ring injury: bilateral anterior pubic root fractures and a disruption of the left sacroiliac joint—61-B2.2
Pelvis, acetabulum: both-column acetabular fracture—62-C2 and 62-C7 body fracture
Femur, proximal: extraarticular fracture, intertrochanteric—31-A3 and wedge diaphyseal fracture—32-B1
Tibia and fibula, proximal: intraarticular bicondylar fracture, no metadiaphyseal involvement—41-C3
Tibia and fibula, shaft—introduction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


