Sterile Instruments/Equipment
- 2.5- or 4.0-mm Schanz pins for use as joysticks in the femoral head/neck fragment.
- Large pointed reduction forceps.
- Modified (straightened) tines for engagement in drill holes.
- Small pointed reduction forceps.
- Modified (straightened) tines for engagement in drill holes.
- Small fragment drill to assess for the vascularity following reduction.
- 5.0-mm Schanz pins for rotational control of distal (shaft) fragment.
- 5/64 inch (2.0-mm) K-wire for use as a distal traction pin with a tensioned traction bow.
- Implants.
- 6.5-, 7.0-, or 7.3-mm fully threaded and partially threaded screws for subcapital/transcervical fractures and hip screw for basicervical fractures.
- Reconstruction and/or mini-fragment plates for provisional stabilization of anteromedial femoral neck in comminuted fractures.
- Bone graft for comminution.
- 6.5-, 7.0-, or 7.3-mm fully threaded and partially threaded screws for subcapital/transcervical fractures and hip screw for basicervical fractures.
Positioning
- Supine on radiolucent table with C-arm from opposite side of the table.
- A small rolled towel bump under the injured hip allows for lateral imaging of hip.
- A bump may not be necessary, as long as fluoroscopic visualization on a cross-table lateral is possible.
- Elevate the operative lower extremity on the leg ramp.
- This relaxes the hip flexors and minimizes deforming forces.
- To increase the hip flexion and offset muscular forces, a radiolucent tibial nailing triangle may be placed under the knee.
- This relaxes the hip flexors and minimizes deforming forces.
- Isolate the perineum from the operative site with an exclusionary drape.
- Sterilely prepare and drape the entire leg circumferentially for maximum control during reduction.
- Sterile skeletal traction using table attachment or dedicated fracture table may facilitate reduction.
Reduction and Fixation Techniques
- Closed reduction attempt by Ledbetter or other femoral neck fracture reduction maneuver.
- Hip flexion, external rotation and abduction followed by gentle traction with hip in flexion.
- Subsequent hip extension and internal rotation may result in an anatomic-appearing reduction on fluoroscopy.
- However, this frequently underestimates the amount of residual displacement that is found upon direct visualization following capsulotomy.
- Hip flexion, external rotation and abduction followed by gentle traction with hip in flexion.
- Closed reduction reserved for subcapital fractures primarily, especially in the geriatric population.
- If closed reduction is deemed acceptable (preferably anatomical on orthogonal and oblique views), consider percutaneous fixation with a decompressive capsulotomy to release the hematoma and to theoretically decrease intracapsular pressure, potentially decreasing the avascular necrosis risk.
- An anterior capsulotomy can be performed utilizing a small laterally based skin incision, with a scalpel blade advanced proximally along the anterior femoral neck.
- C-arm localization is helpful.
- Consider using a disposable scalpel, with the blade integrated into the handle, to prevent disengagement of blade from knife handle, in the stout soft tissues.
- An anterior capsulotomy can be performed utilizing a small laterally based skin incision, with a scalpel blade advanced proximally along the anterior femoral neck.
- Either an anterolateral or an anterior approach can be useful for visualization and reduction of the femoral neck fracture.
- If a Watson-Jones (anterolateral) approach is used, reduction and implant placement can proceed through the same incision.
- However, visualization of the neck fracture and soft tissue retraction is more difficult.
- If a Watson-Jones (anterolateral) approach is used, reduction and implant placement can proceed through the same incision.
- A modified Smith-Petersen (Heuter) approach allows excellent visualization of the anterior femoral neck for reduction and clamp placement (Fig. 13-1).
- A second, small lateral approach is necessary for implant placement if an anterior approach is used.
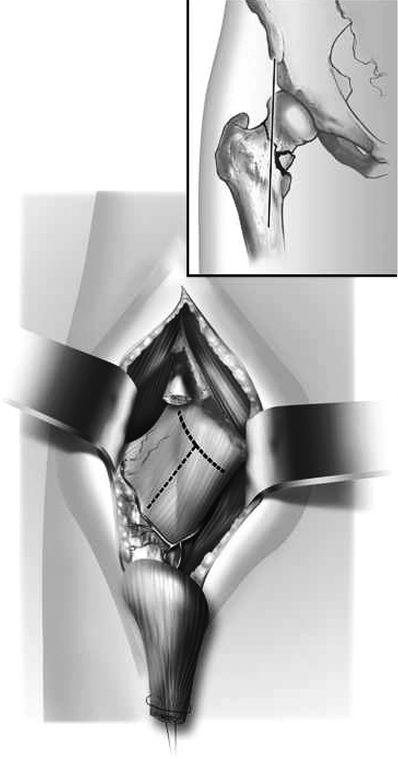
Figure 13-1. These illustrations of a right hip anterior exposure demonstrate the retraction of the sartorius and the iliopsoas muscles medially and the lateral retraction of the tensor fascia lata muscle. The rectus femoris tenotomy is shown, and the planned oblique T-shaped capsulotomy is indicated by the dotted lines. (Adapted from Molnar RB, Routt ML Chip. Open reduction of intracapsular hip fractures using a modified Smith-Petersen surgical exposure. J Orthop Trauma. 2007;21(7):490–494. With permission.)
![]()
- Additional exposure can be achieved by
- Detaching the rectus femoris tendon origin.
- Flexion of the hip by placing a triangle under the leg to relax the rectus, psoas, and sartorius muscles (Fig. 13-2).
- Detaching the rectus femoris tendon origin.

Figure 13-2. The anterior hip capsulotomy has been made, preserving the local vascular anatomy and the anterior labrum. The manipulative reduction screws are shown. (Adapted from Molnar RB, Routt ML Chip. Open reduction of intracapsular hip fractures using a modified Smith-Petersen surgical exposure. J Orthop Trauma. 2007;21(7):490–494. With permission.)
![]()
- Sharp elevation of iliocapsularis may minimize development of heterotopic ossification rather than blunt removal with an elevator.
Related posts:

Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


