External Fixation of Distal Radius Fractures
Introduction
External fixation is an option for fixation of distal radius fractures alone or in conjunction with other fixation techniques
External fixation may be applied in a spanning fashion, crossing the radiocarpal joint; or a nonspanning construct, in which the entire construct is placed on the radius and does not span the radiocarpal joint
One advantage of external fixators is that they can easily be removed after bony healing in the office without a second surgical procedure
Patient Selection
Indications
Failed closed reduction—More than 2 to 3 mm loss of radial length, articular tilt >5° to 10°, radial inclination <10°
Unstable distal radius—Patient older than 60 years, dorsal tilt greater than 20°, dorsal cortex comminution, intra-articular extension, ulna fracture, metaphyseal comminution, ulnar variance
Radiocarpal incongruity greater than 1 to 2 mm
At least 1 cm intact volar cortex for pin purchase
High-grade open distal radius fractures
Initial treatment of polytrauma patient
Always consider patient hand dominance, occupational requirements, medical comorbidities, and expectations
Contraindications
Volar or volar shear displacement pattern
Dorsal shear displacement pattern
Diagnostic Imaging
Radiography
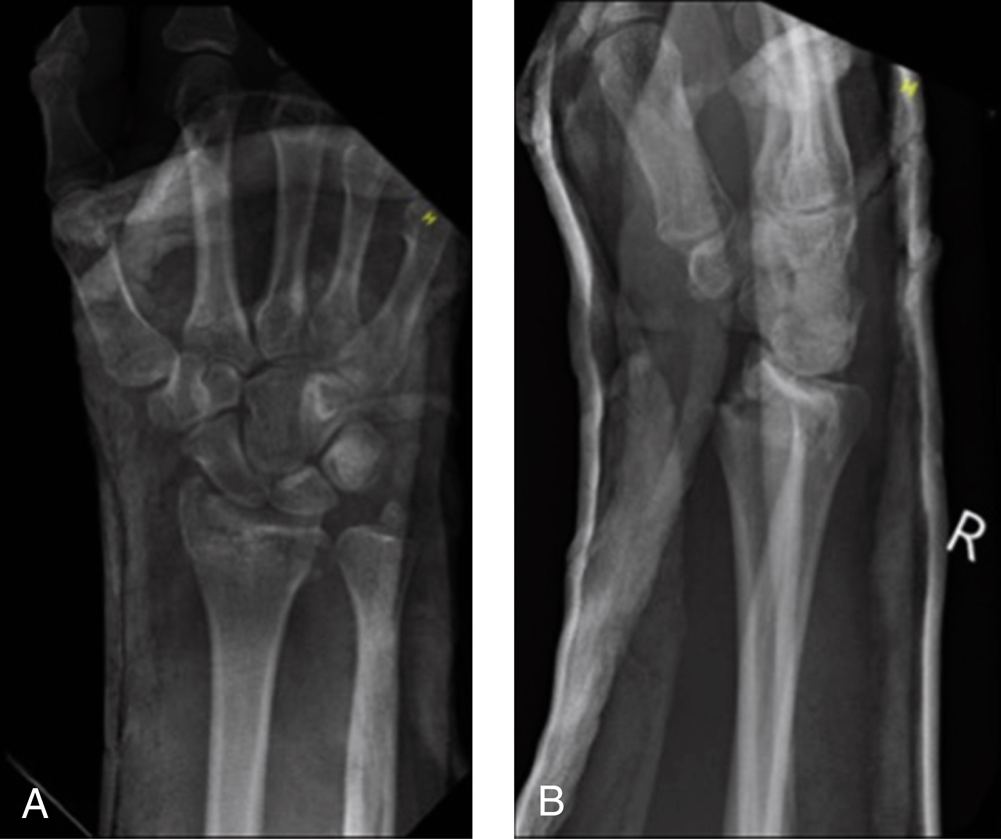
Figure 1AP (A) and lateral (B) radiographs show an AO 23-C2.1 distal radius fracture before reduction.
(Courtesy of Columbia University Medical Center, New York, NY.)
AP, lateral, oblique (Figure 1)
Obtain before and after reduction
Imaging of contralateral wrist helps determine normal anatomy
Traction views can clarify fracture fragments
Computed Tomography
Delineates bony anatomy
Cost and lack of traction limit utility
Procedure
Room Setup/Patient Positioning
Supine position with arm on hand table
Regional or general anesthesia
Nonsterile tourniquet to upper arm set to 250 mm Hg
Prophylactic antibiotics
C-arm or mini C-arm fluoroscopy
Surgical Technique
Perform closed reduction with manipulation as well as traction and countertraction
Choose spanning or nonspanning fixator
If large distal fragment (>10 mm) present, may use nonspanning fixator; articular comminution not absolute contraindication, but half-pins must be centered in fragments; otherwise, use spanning fixator
May use Kirschner wires (K-wires) as joysticks for fragment manipulation
Percutaneous or limited open reduction is possible through 3-cm dorsal incision (between third and fourth compartments); enhance reduction quality and stability with K-wires, impaction grafting of metaphyseal void, arthroscopy or other tools as indicated
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


