CHAPTER 33 Mark E. Easley and Giles R. Scuderi Extensor mechanism insufficiency with: 1. Complete ruptures 2. Partial ruptures 3. Chronic ruptures 1. Functional extensor mechanism (no extensor “lag”) 1. History and physical examination 2. Knee radiographs a. Lateral—to identify patella baja (quadriceps rupture) or patella alta (patella tendon rupture) b. Consider obtaining comparison radiographs of the contralateral knee. 1. Other imaging studies a. MRI is often useful in identifying discontinuity in tendon substance if diagnosis is in doubt or if partial tear is present. 1. Supine position 2. If extremity tends to externally rotate, place a “bump” under the ipsilateral hip. 3. General, spinal, or epidural anesthesia a. Relaxes muscles to facilitate repair b. Permits tourniquet use 4. Intravenous antibiotics 5. Standard instrument set 6. Nonabsorbable suture (#5) 7. Drill 8. Keith needle 9. Suture passer 10. Beath needle 11. Pneumatic burr 12. Cerclage wire 13. Nonabsorbable tape (such as mersilene tape) 14. Intraoperative fluoroscopy or X-ray 15. Tendon stripper (if patella tendon repair warrants augmentation with the semitendinosus or gracilis) 1. Universal vertical midline incision a. Allows adequate exposure b. Functional incision if future surgery is needed 1. Place a tourniquet as proximal as possible on the thigh. 2. Remember to perform a meticulous retinacular repair. 3. Use a Krakow suture technique (interlocking stitch) to ensure adequate purchase of the suture in the tendon. 4. Beath needle a. Use to pass suture through patellar tunnels (in lieu of drilling) and then passing a Keith needle or suture passer b. Saves a step and minimizes the difficulty of finding the tunnel after drilling 1. Tendon stripper (in the event that patella tendon repair requires augmentation with the semitendinosus or gracilis) 2. If necessary, consider a lateral release to improve patella tracking. General principles: 1. If skin contamination is present secondary to either an open injury or skin abrasion, then delay internal fixation until the wound is clean. 2. Avoid creating multiple layers. Attempt to create two full-thickness tissue flaps medially and laterally. 3. If possible, avoid prolonged operative delay. Aim for surgery within the first 10 to 14 days after injury. 4. Avoid reattaching the tendon on the anterior aspect of the patella (this leads to tilt of the patella with tension). 5. Avoid overtightening the patella tendon repair (will create a patella infera). Check intraoperative fluoroscopy or knee X-ray at 45 degrees of flexion; the inferior pole of the patella should be superior to the roof of the intercondylar notch. 1. A suction drain for 24 hours may avoid hematoma. Compressive dressing for 24 to 48 hours is also useful. 2. Immobilize for 4 to 6 weeks in either a knee immobilizer or cylinder cast. 3. Weight bearing as tolerated with knee immobilized in extension 4. Weight bearing may actually reduce the forces across the quadriceps when compared to forces required to support the limb in non-weight bearing. 1. Position patient supine on the operating room table. Place thigh tourniquet as proximal as possible on the thigh. 2. Prepare and drape the limb in the hospital’s standard sterile fashion. Exsanguinate the limb and inflate the tourniquet. 3. Make an anterior skin incision utilizing a straight midline incision. Dissect directly down to the extensor mechanism while minimizing skin flaps. a. Debride damaged tissue back to normal-appearing tendon. However, avoid excising too much tissue. b. Repair end-to-end using #2 or #5 nonabsorbable sutures (interrupted). c. Repair the retinaculum with a nonabsorbable or absorbable #0 suture. d. If necessary, perform a lateral release to improve patellar tracking. e. If repair is tenuous, reinforce repair with a cerclage wire or nonabsorbable tape (such as mersilene tape). f. Proximally, pass the reinforcing wire or tape transversely through the quadriceps tendon. g. Distally, pass the reinforcing wire or tape transversely through a drill hole in the patella.
Extensor Mechanism Injuries
Quadriceps Ruptures and Patella Tendon Ruptures
Indications
Contraindications
Preoperative Preparation
Special Instruments, Position, and Anesthesia
Tips and Pearls
What To Avoid
Postoperative Care Issues
Operative Technique
Approach
Quadricep Tendon
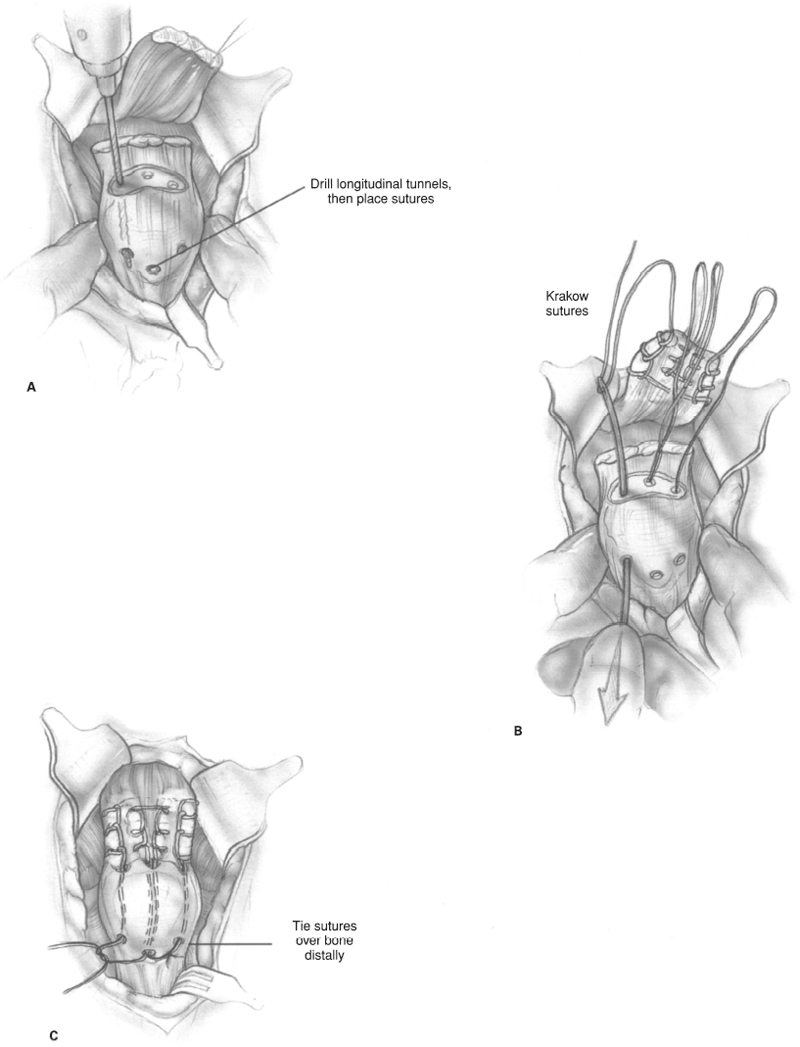
Acute ruptures quadricep tendon (mid-substance)
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


