Ethical issues in chronic care
Objectives
New terms and ideas you will encounter in this chapter
chronic condition
chronic care team
experimental treatment
Topics in this chapter introduced in earlier chapters
| Topic | Introduced in chapter |
| Ethics committee and ethics consultation | 1 |
| A caring response | 2 |
| Locus of authority problem | 2 |
| Moral distress | 3 |
| Quality of life | 3 |
| Utilitarianism | 3 |
| Principles approach | 3 |
| Nonmaleficence | 3 |
| Beneficence | 3 |
| The health care team | 9 |
| Communication | 9 |
| Shared decision making | 11 |
| Informed consent | 12 |
| Assent | 12 |
Introduction
With more than 100 million people in the United States who have at least one chronic condition, chronic care is demanding the attention of health professionals, families, and the health care system more than ever before.1 Many factors contribute to the increase in the number of chronic conditions and symptoms when compared with even a few years ago. Among these are advances in neonatal intensive care, the increasing incidence rate of long-term survival after traumatic brain injury occurring anywhere across the life span, and an increase in adult longevity. These are just some sources of this growing population of patients nationally and globally.
The term chronic condition (from kronos, which means “time” in Latin) focuses attention on long-term management of a condition in contrast to one that is either quickly addressed or is at the end of life. It does not denote that the person eventually will die of the condition, although some do. Examples of the latter include cystic fibrosis, amyotrophic lateral sclerosis, muscular dystrophy, multiple sclerosis, Parkinson’s disease, Huntington’s disease, and severe chronic obstructive pulmonary disease. The common denominator in chronic conditions is that the symptoms persist over time, some for months, years, or a lifetime. You may know someone (or be a person) with one of the previous conditions or someone who lives with symptoms of arthritis, diabetes, clinical depression, schizophrenia, dyslexia, or one of the dementias. The presence of all these forms lends support to the idea that in your generation of the health professionals, most of you will be deeply involved in the treatment of chronic symptoms and the functional impairment that often accompanies them. Currently, the clinical management of patients with chronic conditions often lacks coordination among specialties, providing plenty of room for you to become advocates for improving the quality of care for such persons.2 This chapter focuses directly on the ethical challenges this population presents and relevant details for achieving a caring response to this condition. A caring response is not unique in comparison with other types of conditions, but at times, the challenges present in slightly different forms. It is noteworthy that in almost all chronic conditions the patient interacts with a whole team of people, sometimes with a chronic care team specifically, but other times with teams devoted to a particular disease or injury. This in itself creates an environment of multiple relationships that affect the patient and, very often, include the family or others who provide care besides health professionals.
Reflection

Do you have a friend, family member, or colleague who has a chronic condition that necessitates ongoing clinical interventions? Perhaps you have one yourself. What are the major challenges that you think, or know, face this person? Are there disruptions in everyday activity that they experience? How are their daily routines different from others’? Jot down a few notes so that as you go through the chapter you can relate that person’s situation back to the opportunities health professionals have to provide patient-centered care.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
As you have experienced in previous chapters, to further help set your thinking, you have an opportunity to examine a narrative, this one of a family who is interacting with the health care system because one family member is in a situation that requires ongoing care.
The Story of the McDonalds and the Cystic Fibrosis Team

The pregnancy had been without complication, and the delivery was much easier than Megan had imagined it would be. She and Gerald beheld the screaming newborn with the wonder that only new parents can feel. Mary Elizabeth McDonald had entered this world with all the gusto her parents presumed she would need as a second-generation immigrant in their adopted land.
And so it came as a shock to parents and clinical staff alike when shortly after her birth Mary Elizabeth had serious respiratory distress develop. She was placed in the pediatric intensive care unit, and after several series of tests, the clinicians told her parents that Mary Elizabeth had cystic fibrosis. The parents asked many questions about this condition, and nothing they heard sounded encouraging. Gerald went online to find out all he could from the Internet, which plunged them into despair. The health care team in the intensive care unit, including a genetic counselor, social workers, and others, tried to console and encourage them, highlighting the great strides in treatment and longevity that individuals with this incurable chronic condition have enjoyed in the past several years. But Megan and Gerald feared that they had brought this long-awaited and beloved child into the world to endure a life of suffering if, indeed, Mary Elizabeth lived beyond infancy.
That was 12 years ago. Today, Mary Elizabeth is a bright, beautiful child, small and thin for her age, but with a happy spirit. Her inner vitality is a joy to all that meet her, although her life includes long periods of hospitalization and home schooling (and treatment) because of the seriousness of her symptoms. She begins and ends each day with bouts of severe coughing, sometimes for an hour at a time, and several times she has had bacterial infections and pneumonia so serious that the family’s parish priest has administered the sacrament of Last Rites, provided only for persons who are believed to be imminently dying. Her school schedule is arranged so that only a few of her classmates surmise where she goes when she leaves daily for the school clinic for the vigorous chest percussion needed to loosen the thick brown mucus that continuously gathers in her lungs. The entire family agrees that it was worth the expense to move to a larger city where they have access to the ongoing availability of an excellent cystic fibrosis team. Given their repeated encounters with the health care system, they find it a wise choice. Among the most helpful is team member Betty Mortimer, a respiratory therapist whose own family has a history of cystic fibrosis and who has been on the team treating Mary Elizabeth for years.
Mary Elizabeth excels in school and is seen as a leader among her peers. Over the years, all three McDonalds have learned to live a day at a time to see what it holds for them as a family. Some days, Megan’s activities are completely given over to tending to Mary Elizabeth; other times, she almost forgets that there is any difference between her daughter and other children. Gerald has taken a second job to help defray expenses. Currently, both parents are concerned that Mary Elizabeth is entering puberty and fear that the teen years will present her with new challenges exacerbated by her chronic symptoms. They have long belonged to a parent support group and know that some young people with cystic fibrosis have less difficulty than others making the transition into the teen and adult years, succeeding in their social life and studies, having satisfying careers, and finding a life partner. They also have learned more about the genetic component of cystic fibrosis and know that soon they will have to discuss with her the probabilities of her own children having the condition or being carriers of it. Given their strong religious position on abortion, Megan was shocked to overhear Mary Elizabeth say to a friend recently, “If I got pregnant, I’d have to have an abortion so my child wouldn’t have to go through what I’m goin’ through.” Megan wept all day.
Unbeknown to the McDonalds, the cystic fibrosis team is having a crisis of its own. The head pulmonary specialist on the team, Dr. Abraham Levy, who has managed Mary Elizabeth’s care for 8 years, is a world-renowned expert in the field. He announces to the team that he plans to persuade the family to put Mary Elizabeth on an experimental treatment in the form of an intravenous medication that the team has used in two other cases rather than having her undergo a lung transplant. The experimental treatment has passed the test of safety and effectiveness standards set by the federal government and has been tested on animals. Now it is being attempted on select patients as part of a phase II clinical trial. A visible pall falls over the room. Three members of the eight-member team assent to his decision, but the second most experienced physician on the team begins to argue with Dr. Levy about this decision. What all of them know is that although this experimental intervention has been heralded in reputable journals and medical circles as a “miracle drug,” decreasing the rate of breakdown of the respiratory system in some patients, the first time it was attempted at this institution the patient died shortly after the treatment was administered. Since then, two additional serious deleterious responses to the drug have been reported in the literature. Dr. Levy says that Mary Elizabeth so perfectly fits the criteria for inclusion in the clinical trial that he feels confident of its success and on that basis, the patient’s informed consent will be easy to obtain. Some of the team conclude that he will emphasize the benefits of the drug choice only and overemphasize the (to be sure) serious risks of a lung transplant option for the patient.
The next day, Dr. Levy announces to the team that he raised the issue with the McDonalds and obtained their informed consent. Mary Elizabeth was there, assented, and was very excited. “Maybe I can play soccer like my friends!” he reported her as saying. Although the McDonalds were more cautious, he relayed, they decided to go ahead, hoping that she might be among the first to benefit from this new intervention. Mary Elizabeth mentioned also maybe being able to help other girls like herself who will suffer from the effects of cystic fibrosis in the future. Looking around the room and seeing their questioning eyes, Dr. Levy says, “Come on, you doubters. We all have the same goals in mind, and we have to pull together!”
After the team meeting that day, the five members who question Dr. Levy’s decision lag behind in the lounge. To put it lightly, they are very upset and unsure of what to do. They pride themselves in being a well-working team and have great respect for Dr. Levy and each other. They have traditionally made such decisions as a full care team. Betty in particular is concerned as she recalls Mary Elizabeth saying that she saw a television program where some doctors were experimenting on patients behind the patients’ backs and that of all the things she could not handle, it would be that. They tried to assure her that situation seldom happens and is completely unethical. It would not happen to her here. She could count on that. They are aware that Dr. Levy has little time for what he calls the “armchair philosophers” on the ethics committee, and he prides the team in being able to work out their differences in a reasonable and respectful manner. So he will be upset with them if his decision goes to the ethics committee, an alternative one of them suggests. Another member thinks in this case it is appropriate for each of them to do more research on their own, both about the effects of the experimental medication and also about what the McDonalds were told. Because the treatment is not scheduled to begin until the next week, they agree to all go home and sleep on it and then reconvene after work the next day.
This care team, the patient, and the family are in a relationship that is not unusual for patients with chronic conditions. Some characteristics of this type of team relationship are:
• the shared concern for and loyalty to the patient;
• the long experience of working with each other;
• knowledge that the family caregivers are very much affected by the patient’s condition; and
In addition, the complexity and uncertainty facing all of them about what to do next is not unusual. Chronic, long-term conditions always continue to evolve over time, unlike more acute conditions. We turn now to the challenges they face together.
The goal: a caring response
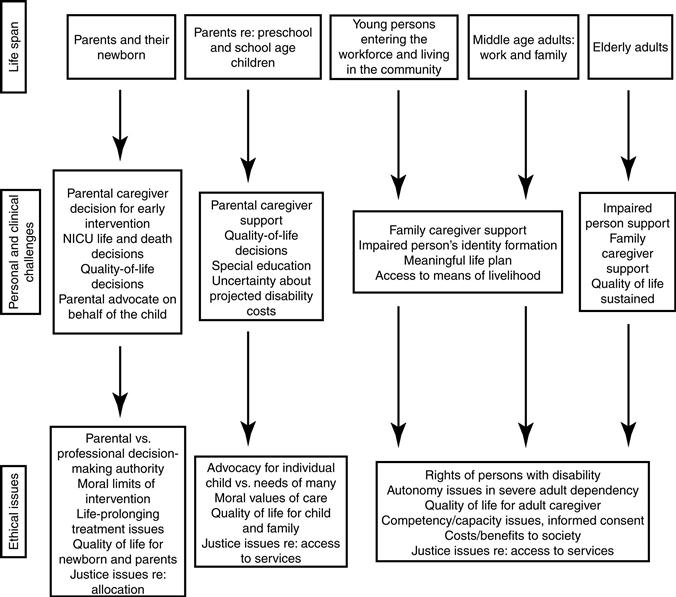
The means by which the goal of a caring response in this situation can be realized is, in many regards, similar to those in any other type of situation. For instance, the care must be personalized to the needs of the patient’s specific situation. However, as we already noted, a key consideration that distinguishes a chronic care situation from many others is that collectively the interventions extend over a long period, sometimes from the patient’s birth to her or his adulthood and old age. Figure 13-1 outlines several dimensions of the range and possible lifelong duration of chronic conditions.
We can predict that in Mary Elizabeth’s case, she (and until she reaches adulthood, her parents) will be in relationships with health professionals on a regular basis. For her, there is a high probability this will continue throughout her entire life.3
There also are several generic considerations that apply to all patients with chronic conditions.
First, for most patients, their expectations of the health professional or team is not to effect a cure, although if a cure would become known, the focus obviously should shift in that direction.
Second, the point of accepting clinical interventions is to protect or improve the quality of life, whether it be through prevention of secondary symptoms, freedom from pain or other discomfort, or rehabilitation designed to help build or sustain important functions, relationships, and roles. The health fostering and health maintenance interventions for the patient with one ongoing condition (complete with its evolving symptoms over months or years) casts the challenge in a somewhat different light than those directed to acute symptoms. It is a balance of periods of illness and wellness. Persons with a chronic condition have been found to experience challenges to life meaning, needing to balance freedom to do as they want and feel they need to do with loss of control.4
Third, and related to the second, the patient counts on the professionals to design treatment programs with the idea that the family (or other significant personal caregiver) is an essential consideration. More than in most other types of treatment planning, the health professional team must take the family caregivers’ well-being into account (see later for further discussion of this point). In Mary Elizabeth’s or other children’s situations, a parent or other adult guardian is the legal spokesperson. The same is true for adults with limited capacity, as discussed in Chapter 12. There are not only ethical but also economic and other practical reasons for making decisions that are appropriate for the family caregivers’ needs, and the patient’s.5
Fourth, clinically and socially, the patient needs the professionals to be acutely aware that “the chronically ill” may have difficulty harnessing appropriate long-term care services. A caring response on the part of the professional must include concerted advocacy efforts designed to counteract and denounce such discrimination and dehumanizing experiences. This extended role of the health professions is discussed in Section V of this book.
Reflection

Can you think of other considerations that should inform health professionals who are working with chronic conditions but might not be as important in acute care settings? List them here.
Summary

In chronic condition situations, a factor that affects treatment decisions is that cure often is not the goal, whereas quality of life is.
Again, the six-step process of ethical decision making can be called on for assessing and discerning an ethical course of action in chronic care situations.
The six-step process in chronic care situations
Let us return to the McDonalds and the cystic fibrosis team; we pick up the story at the juncture where the team has become divided about the decision made by the team leader. The first step is to gather relevant information.
Step 1: gather relevant information
The team is paying attention to information that has caused them concern. They know that the drug has been approved for human use in selected situations, such as Mary Elizabeth’s case, and that the alternatives for Mary Elizabeth are few. They know all too well that a lung transplant is a high-risk surgery and that for some patients the symptoms of cystic fibrosis grow more serious during the changes of puberty and adulthood.
Evolving clinical status over time
Unlike most health professionals who work in acute care situations, the chronic care team (in this case, the specialized cystic fibrosis team) is in a position to assess a patient’s status over a period of time. The members have been working with the McDonalds for several years; therefore, they have a reasonable understanding of Mary Elizabeth’s current clinical condition compared with previously. Her condition can be characterized as stable, with the only big unknown being the patient’s prepubesence; however, they can compare her condition with conditions of other similarly situated patients because their clinical expertise is in cystic fibrosis and respiratory disease.
Like many teams, they are now faced with a situation in which their certainty is faltering. They know that so far the team has been able to help the McDonalds manage Mary Elizabeth’s symptoms. Unfortunately, at this pivotal moment in the team’s relationship, they themselves are divided because of the uncertainty of what is best for Mary Elizabeth, a challenge that so often creates distress for teams working with chronic conditions. Their firsthand experience with the proposed course of action for Mary Elizabeth is limited to the serious negative outcome it had for their one other patient on the unit, an 8-year-old child. They will have to do their homework regarding this ongoing clinical trial and also regarding the surgical option of lung transplant. Is the experimental approach appropriate for a young patient just entering puberty? There is no evidence of long-term effects because the intervention is so new. How does this weigh in the decision?
Team effects
Fortunately, overall the professionals believe they are privileged to work with a group of outstanding colleagues in this field of medicine, at one of the world’s top academic medical centers specializing in respiratory and pulmonary disease. The team is a “dream team” (most of the time!), hitting the rough spots with their common goals to guide them and with deep respect for each other’s competence.
It is relevant information that similar to most chronic care situations, the family caregivers have developed a deep trust in the team as a unit. The family must feel free to raise questions, express their emotions, and in other ways show their concern within the current situation. When this trust breaks down, the negative effects on the family may haunt them for years.6 For the McDonalds’ well-being, all activity should be pursued in a manner that allows that trust to be sustained, no matter the actual treatment approach, experimental or transplant. This, of course, means the team be totally trustworthy (Figure 13-2).

Related posts:
 Surviving student life ethically
Surviving student life ethically
 Ethics theories and approaches: conceptual tools for ethical decision making
Ethics theories and approaches: conceptual tools for ethical decision making
 Morality and ethics: what are they and why do they matter?
Morality and ethics: what are they and why do they matter?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


