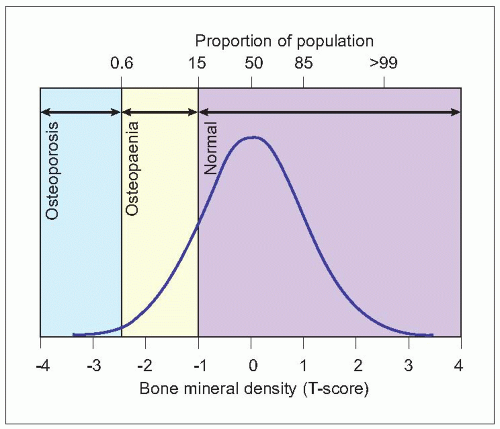
 2.1 Distribution of bone density in healthy women aged 30-40 years. (Adapted from WHO (2003). Prevention and Management of Osteoporosis. WHO Technical Report Series No. 921. World Health Organization, Geneva.) |
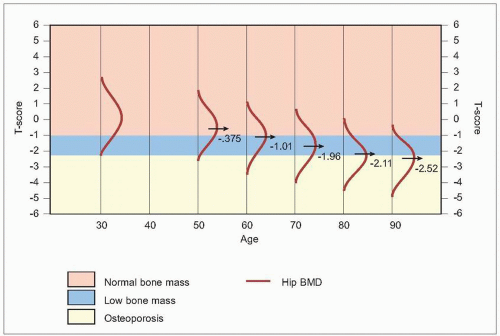 2.2 The distribution of bone density at increasing ages. (Adapted from Kanis J, et al. (1994). The diagnosis of osteoporosis. J Bone Mineral Res 9(8):1137-1141.) |
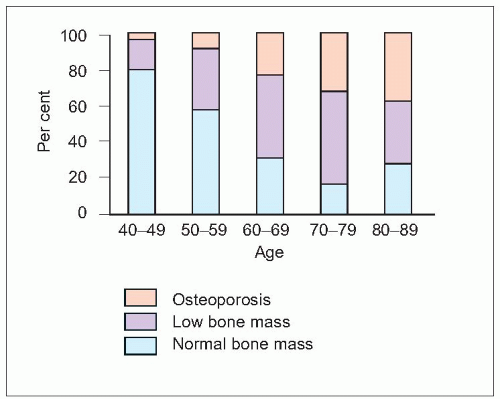 2.3 The percentage of women in Sweden with normal bone mass, low bone mass, and osteoporosis in the hip at increasing ages. (Adapted from SBU (1995). Measurement of bone mineral density. SBU Report 127. Swedish Council of Technology Assessment in Health Care, Stockholm.) |
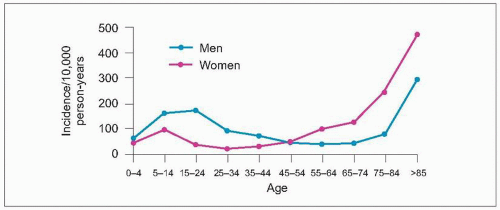 2.4 Incidence of fractures in the UK. (Adapted from Donaldson LJ, et al. (1990). Incidence of fractures in a geographically defined population. J Epidemiol Community Health 44(3):241-245.) |
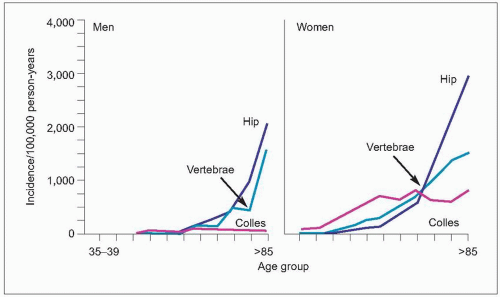 2.5 Incidence of the major age-related fractures in men and women. (Adapted from Cooper C, Melton LJ (1992). Epidemiology of osteoporosis. Trends Endocrinol Metab 314:224-229.) |
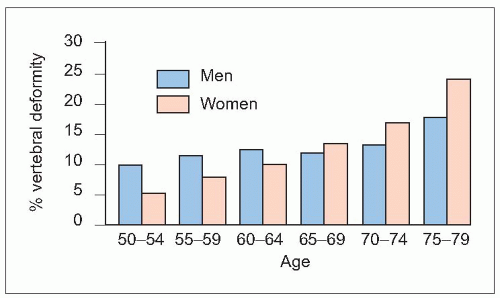 2.6 Age distribution of vertebral fractures. (Adapted from O’Neill TW, et al. (1996). The prevalence of vertebral deformity in European men and women: the European Vertebral Osteoporosis Study. J Bone Mineral Res 11(7):1010-1018.) |
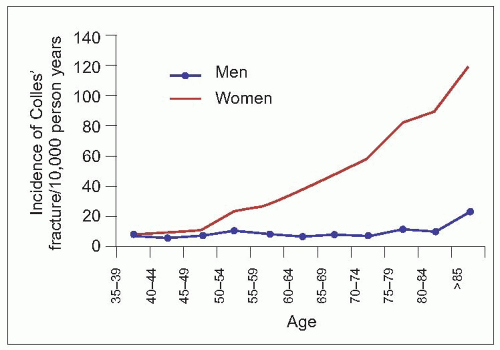 2.7 Age distribution of distal forearm fractures. (Adapted from O’Neill TW, et al. (2001). Incidence of distal forearm fracture in British men and women. Osteoporos Int 12(7):555-558.) |
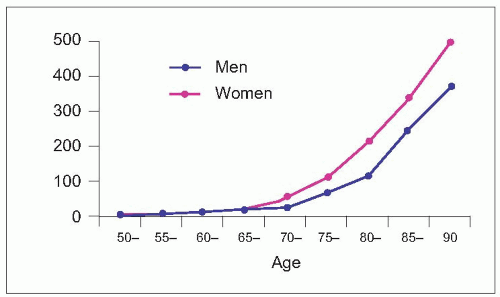 2.8 Age distribution of hip fractures. (Adapted from Rogmark C, et al. (1999). Incidence of hip fractures in Malmö, Sweden, 1992-1995. A trend-break. Acta Orthop Scand 70(1):19-22.) |
Table 2.1 Incidence of hip fracture (rates/100,000) in 1990 by age, sex, and region | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
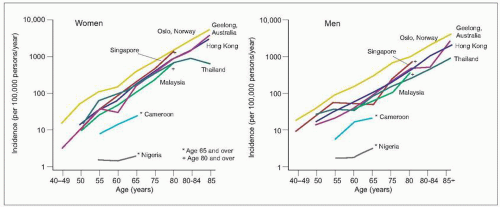 2.9 The age-specific incidence of hip fractures in different countries. (Adapted from Zebaze RM, Seeman E (2003). Epidemiology of hip and wrist fractures in Cameroon, Africa. Osteoporos Int 14(4):301-305.) |
Table 2.2 Estimated lifetime risks of fractures (%) in the UK at various ages | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2.3 Estimated 10-year risks (%) of fractures in the UK at various ages | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2.4 Probability of fracture during the next 10 years in men and women from Sweden (according to age and risk relative to the average population) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
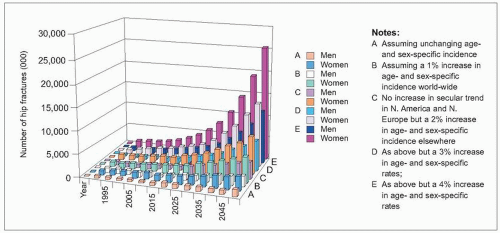
 2.10 Projected number of yearly incident fractures in the European Community member states. (Adapted from European Communities (1998). Report on Osteoporosis in the European Community: action for prevention. European Communities, Luxembourg.) |
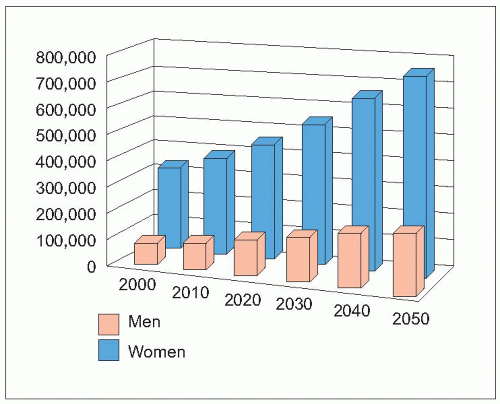
 2.11 Worldwide forecasts for hip fracture, 2050. (Adapted from Gullberg B, et al. (1997). Worldwide projections for hip fracture. Osteoporos Int 7(5):407-413.) |
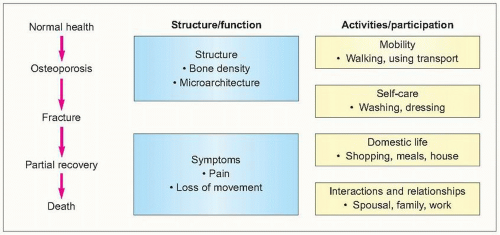 2.12 Impact of osteoporosis in terms of the WHO International Classification of Functioning. |
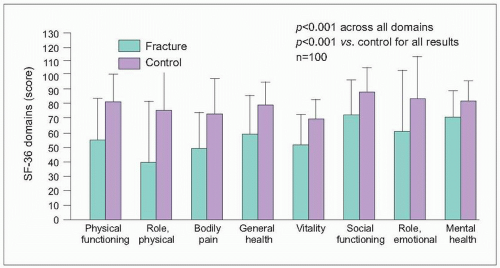 2.13 Vertebral fractures and quality of life. (Adapted from Hall SE, et al. (1999). A case-control study of quality of life and functional impairment in women with long-standing vertebral osteoporotic fracture. Osteoporos Int 9(6):508-515.) |
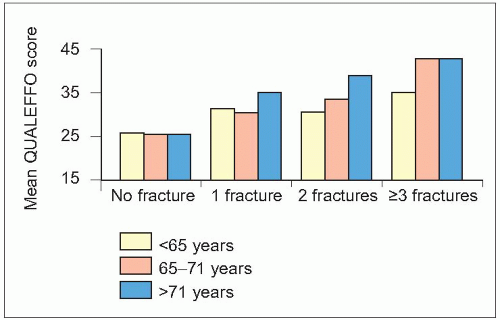 2.14 Impact of age and number of vertebral fractures. (Adapted from Oleksik A, et al. (2000). Health-related quality of life in postmenopausal women with low BMD with or without prevalent vertebral fractures. J Bone Mineral Res 15(7):1384-1392.) |
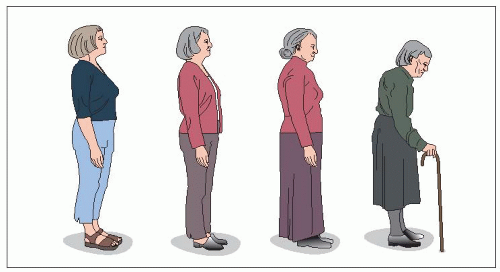 2.15 Progressive loss of height associated with vertebral deformities. |
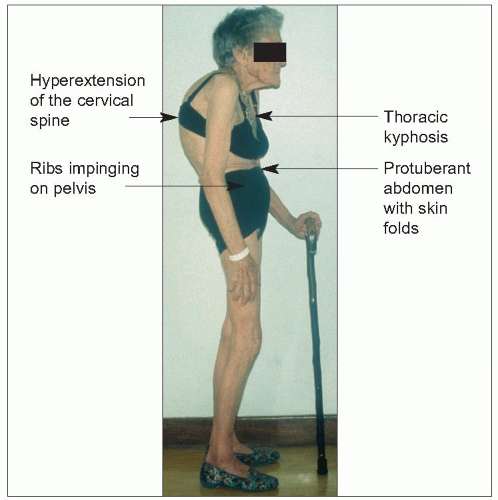 2.16 The clinical problems associated with vertebral osteoporosis and fracture. |
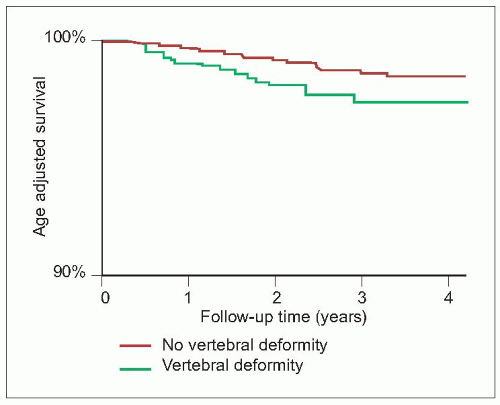 2.17 There is an increased mortality associated with vertebral deformities. Age-adjusted Kaplan Meier survival curves in women. (Adapted from Ismail AA, et al. (1998). Mortality associated with vertebral deformity in men and women: results from the European Prospective Osteoporosis Study (EPOS). Osteoporos Int 8(3):291-297.) |
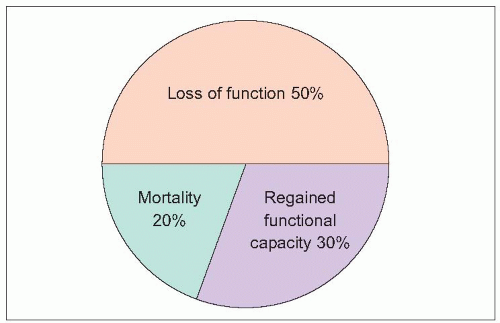 2.18 Outcome after hip fracture at 1 year. (Adapted from Sernbo I, Johnell O (1993). Consequences of a hip fracture: a prospective study over 1 year. Osteoporos Int 3(3):148-153.) |
Table 2.5 Distal forearm fractures (Colles) | |
|---|---|
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


