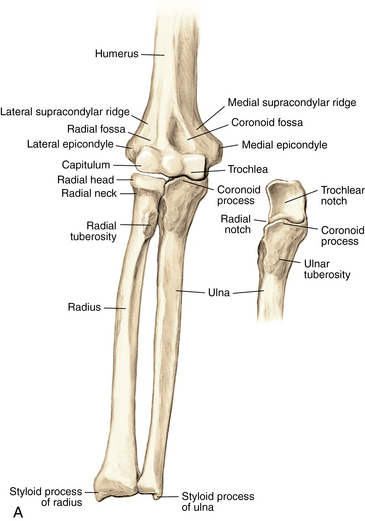
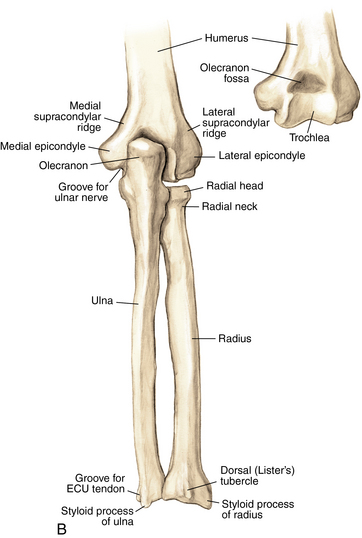
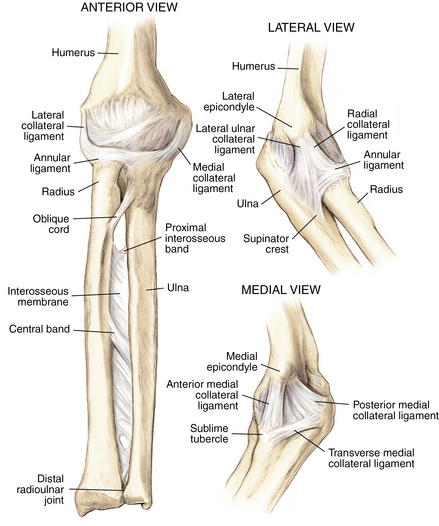
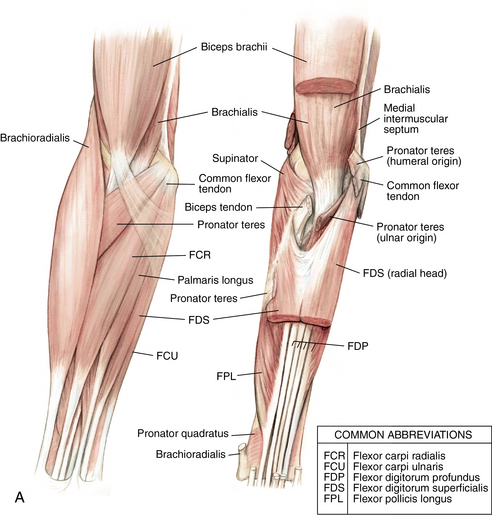
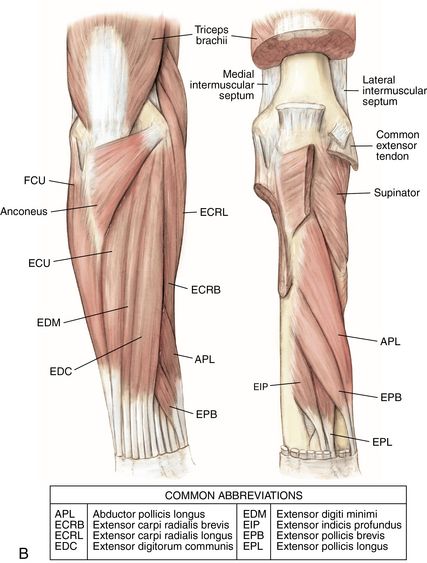
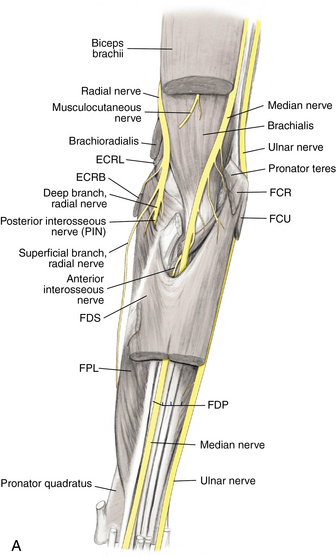
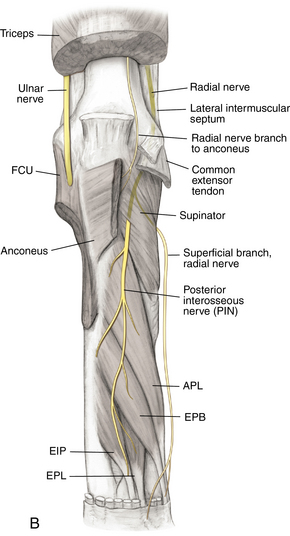
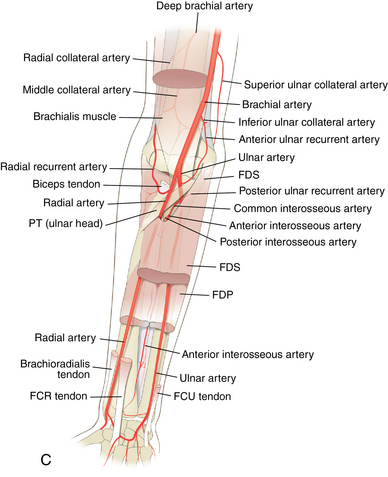
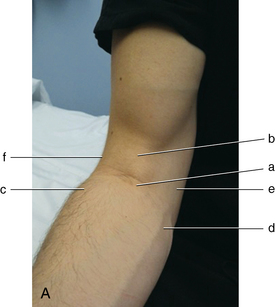
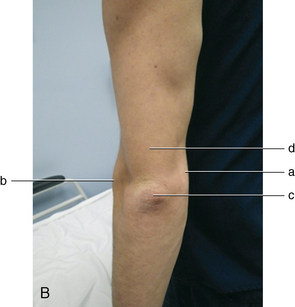
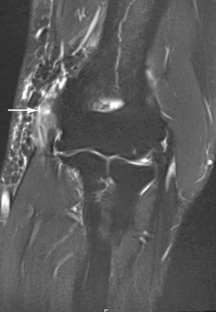
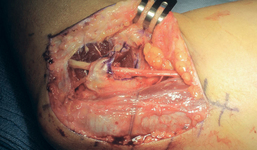
3 Elbow and forearm Figure 3-2. Ligaments of the elbow and forearm. Components of the elbow ligaments—ulnar collateral ligament: anterior band, posterior band, and transverse band; lateral collateral ligament: annular ligament, radial collateral ligament, accessory collateral ligament, and lateral ulnar collateral ligament. (From Chhabra AB: Elbow and forearm. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 67.) Figure 3-3. A, Muscles and tendons of the anterior elbow and forearm: superficial and deep compartments. B, Muscles and tendons of the posterior elbow and forearm: superficial and deep compartments. (From Chhabra AB: Elbow and forearm. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, pp 68, 69.) Figure 3-4. A, Anterior view of the nerves of the elbow and forearm. B, Posterior view of the nerves of the elbow and forearm. C, Arteries of the elbow and forearm. APL, abductor pollicis longus; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; EIP, extensor indicis profundus; EPB, extensor pollicis brevis; EPL, extensor pollicis longus; FCR, flexor carpi radialis; FCU, flexor carpi ulnaris; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; FPL, flexor pollicis longus; PT, pronator teres. (From Chhabra AB: Elbow and forearm. In Miller MD, Chhabra AB, Hurwitz S, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, pp 74, 75, 81.) Figure 3-5. Surface anatomy of the anterior and posterior elbow and forearm. A, Anterior labels: a) antebrachial fossa, b) biceps tendon, c) common extensor tendons, d) common flexor tendons, e) medial epicondyle, f) lateral epicondyle. B, Posterior labels: a) medial epicondyle, b) lateral epicondyle, c) olecranon process, d) triceps tendon. Inspect for edema, deformity, ecchymosis, biceps muscle. Table 3-2. Normal Elbow and Forearm Range of Motion Table 3-4. Differential Diagnosis of Elbow Pain Figure 3-8. Magnetic resonance image of lateral epicondylitis. Edema and high-grade partial tearing of the common extensor tendon origin are visible (arrow). • Perform a wound check and suture removal. • Therapy: Start therapy for gentle elbow ROM. The patient should avoid lifting with the operative extremity. • Perform a motion check. Evaluate and document whether the patient has tenderness to palpation at the lateral epicondyle. Figure 3-9. Magnetic resonance image of medial epicondylitis. Edema and high-grade partial tearing of the common flexor tendon origin are visible (arrow). Medial epicondylitis is also known as golfer’s elbow and is a form of tendinitis. It is an inflammatory condition, and treatment revolves around decreasing the inflammation and strengthening the musculature. Because the tendons that are inflamed are responsible for wrist flexion and pronation, the pain is occasionally worse with gripping, lifting, and twisting. • Perform a wound check and suture removal. • Therapy: Start gentle elbow ROM. The patient is to avoid lifting with the operative extremity. • Perform a motion check. Evaluate and document whether the patient has tenderness to palpation at the medial epicondyle. Figure 3-12. Intraoperative photograph of a transposed ulnar nerve. The nerve now lies anterior to the medial epicondyle and is held in place by lengthened flexor-pronator fascia. • Some clinicians advocate for an early therapy session for gentle elbow ROM and edema control to prevent stiffness. A removable thermoplastic long-arm posterior splint may be fabricated to support the arm between therapy sessions. • Sutures are removed, and ROM is assessed. • Inquire about and document changes in preoperative paresthesias. • Perform a wound check, and evaluate for hypersensitivity. • Inquire about and document changes in preoperative paresthesias. • Check and document Froment and Wartenburg signs. • The patient can start strengthening exercises between 6 and 8 weeks and gradually return to everyday activities without restrictions. Olecranon bursitis is a condition of inflammation or infection of the olecranon bursa. It can occur from repetitive leaning on the elbow or from mild trauma. The bursa can be filled with sterile serous fluid or infection. Recurrences are possible and may require repeat aspiration, but nonoperative treatment is successful most of the time. If the bursitis is mild and clinically deemed to be aseptic, avoid aspiration, to reduce the risk of iatrogenic infection.
Anatomy
Ligaments: Figure 3-2
Muscles and tendons: Figure 3-3
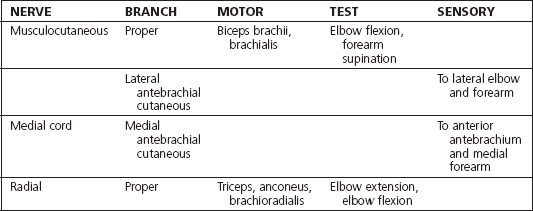
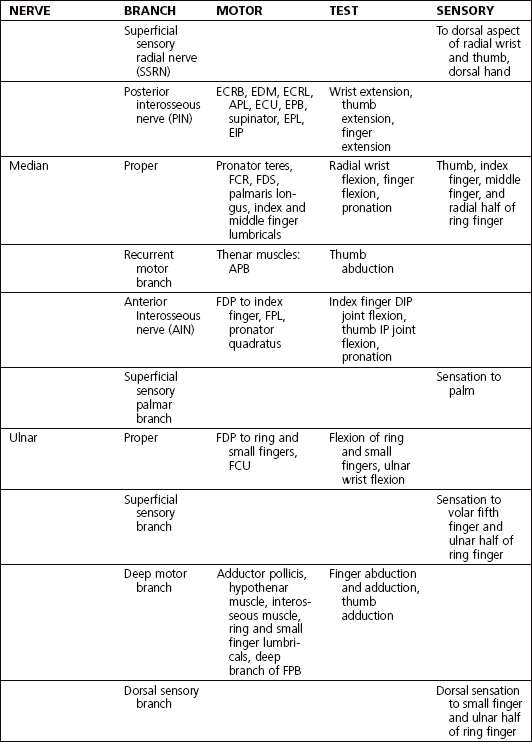
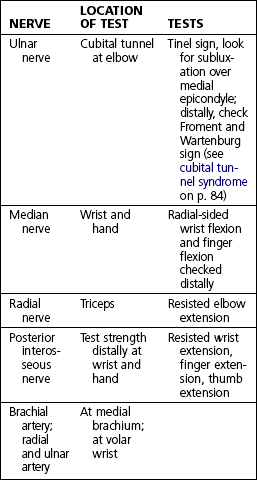
Nerves and arteries: Figure 3-4 and table 3-1
Surface anatomy: Figure 3-5
Physical examination (table 3-2, 3-3, 3-4)
Extension
0 degrees
Flexion
135 degrees
Supination
90 degrees
Pronation
90 degrees
Medial-sided elbow pain
Medial epicondylitis
Ulnar collateral ligament injury
Arthritis
Cubital tunnel syndrome
Lateral-sided elbow pain
Lateral epicondylitis
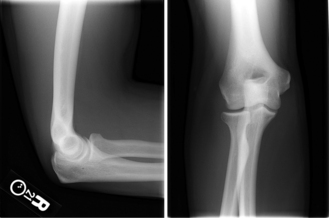
Radial head fracture
Lateral collateral ligament injury
Anterior elbow pain
Biceps tendinitis or biceps tendon rupture
Posterior elbow pain
Olecranon bursitis
Triceps tendinitis
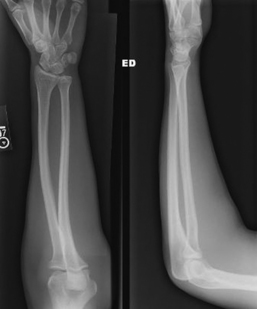
Forearm pain
Radial tunnel syndrome
Muscle strain
Lateral epicondylitis
Imaging: Figure 3-8

Initial treatment
Treatment options
 Conservative management is reserved for patients with no previous treatment or whose previous treatment was successful but the problem recurred after several months or years.
Conservative management is reserved for patients with no previous treatment or whose previous treatment was successful but the problem recurred after several months or years.
 Avoid multiple repeat injections over a short time because they can result in local tissue destruction and possible tendon or ligament rupture.
Avoid multiple repeat injections over a short time because they can result in local tissue destruction and possible tendon or ligament rupture.
 Advise the patient on a period of rest and activity modification after injection.
Advise the patient on a period of rest and activity modification after injection.
Surgical procedures
Lateral epicondyle débridement
Estimated postoperative course
Medial epicondylitis
Physical examination
Imaging: Figure 3-9
Initial treatment
Treatment options
 Conservative management is reserved for patients with no previous treatment or whose previous treatment was successful but the problem recurred after several months or years.
Conservative management is reserved for patients with no previous treatment or whose previous treatment was successful but the problem recurred after several months or years.
 A relative contraindication to injection is a subluxating ulnar nerve.
A relative contraindication to injection is a subluxating ulnar nerve.
 Advise the patient on a period of rest and activity modification after injection.
Advise the patient on a period of rest and activity modification after injection.
Surgical procedures
Medial epicondyle débridement
 An oblique incision is made just anterior to the medial epicondyle. Care is taken to avoid injury to the medial antebrachial cutaneous nerve and ulnar nerve in the cubital tunnel.
An oblique incision is made just anterior to the medial epicondyle. Care is taken to avoid injury to the medial antebrachial cutaneous nerve and ulnar nerve in the cubital tunnel.
 A rongeur or curette is used to débride the dysvascular tissue and to stimulate bleeding. Avoid injury to the underlying UCL. Sometimes, a K-wire is used to puncture the medial epicondyle several times to stimulate bleeding at the origin of the tendon.
A rongeur or curette is used to débride the dysvascular tissue and to stimulate bleeding. Avoid injury to the underlying UCL. Sometimes, a K-wire is used to puncture the medial epicondyle several times to stimulate bleeding at the origin of the tendon.
Estimated postoperative course
Cubital tunnel syndrome
Physical examination
 Tenderness over the ulnar nerve at the cubital tunnel
Tenderness over the ulnar nerve at the cubital tunnel
 Inspection for intrinsic muscle atrophy in the hand, or claw deformity (late finding)
Inspection for intrinsic muscle atrophy in the hand, or claw deformity (late finding)
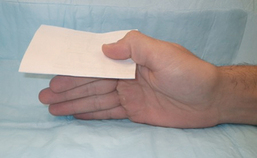
Froment sign: Figure 3-11
 This test evaluates for weakness of the adductor pollicis muscle caused by ulnar nerve injury.
This test evaluates for weakness of the adductor pollicis muscle caused by ulnar nerve injury.
 A positive sign is when the patient flexes the thumb interphalangeal joint and thereby activates the flexor pollicis longus (a median nerve innervated muscle) to hold the paper, instead of using the adductor pollicis.
A positive sign is when the patient flexes the thumb interphalangeal joint and thereby activates the flexor pollicis longus (a median nerve innervated muscle) to hold the paper, instead of using the adductor pollicis.
Initial treatment
Treatment options
Operative management
Informed consent and counseling
Surgical procedures
 Medial approach over the ulnar nerve at the elbow
Medial approach over the ulnar nerve at the elbow
 Ulnar nerve decompression or decompression and transposition of the ulnar nerve
Ulnar nerve decompression or decompression and transposition of the ulnar nerve
Ulnar nerve transposition (subcutaneous or submuscular): Figure 3-12
 Instruments: Vessel loops are used to hold the nerve gently during dissection.
Instruments: Vessel loops are used to hold the nerve gently during dissection.
 Once the nerve has been transposed, the elbow is placed through ROM to ensure that the nerve no longer subluxes with flexion, has no areas of compression, and is not under tension. The wound is then irrigated and the skin closed. A Jackson-Pratt (JP) drain or similar drain may be placed into the wound to be removed before discharge home or on postoperative day 1. Most surgeons place the patient in a postoperative long-arm posterior splint with the elbow at 90 degrees and the forearm in neutral.
Once the nerve has been transposed, the elbow is placed through ROM to ensure that the nerve no longer subluxes with flexion, has no areas of compression, and is not under tension. The wound is then irrigated and the skin closed. A Jackson-Pratt (JP) drain or similar drain may be placed into the wound to be removed before discharge home or on postoperative day 1. Most surgeons place the patient in a postoperative long-arm posterior splint with the elbow at 90 degrees and the forearm in neutral.
Estimated postoperative course
Olecranon bursitis
Physical examination
Initial treatment
Treatment options
 For mild inflammatory bursitis: Suggest ice, NSAIDs, an elbow pad or elastic (Ace) wrap for compression, and avoidance of leaning on the elbow. These treatments may take several weeks to be successful.
For mild inflammatory bursitis: Suggest ice, NSAIDs, an elbow pad or elastic (Ace) wrap for compression, and avoidance of leaning on the elbow. These treatments may take several weeks to be successful.
 For symptomatic inflammatory bursitis:
For symptomatic inflammatory bursitis:Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree