Abstract
Objective
The objective of this trial was to evaluate the effect of gender on strength gains after five week training programme that consisted of isometric exercise coupled with electromyographic biofeedback to the quadriceps muscle.
Materials and methods
Forty-three (20 men and 23 women) patients with knee osteoarthritis (OA), were placed into two groups based on their gender. Both groups performed isometric exercise coupled with electromyographic biofeedback for five days a week for five weeks.
Results
Both groups reported gains in muscle strength after five week training. However, the difference was found to be statistically insignificant between the two groups ( P = 0.224).
Conclusion
The results suggest that gender did not affect gains in muscle strength by isometric exercise coupled with electromyographic biofeedback in patients with knee OA.
Résumé
Objectif
L’objectif de cette étude était d’évaluer les effets liés au sexe pour l’augmentation de force après un programme d’entraînement isométrique du quadriceps de cinq semaines couplé à du biofeedback électromyographique (BEMG).
Patients et méthode
Quarante-trois patients (20 hommes et 23 femmes) atteints de gonarthrose étaient divisés en deux groupes selon leur sexe. Les deux groupes suivaient le même programme de renforcement musculaire isométrique couplé à du BEMG cinq jours par semaine pendant cinq semaines.
Résultats
Les deux groupes montraient une augmentation de la force musculaire après cinq semaines d’entraînement. Cependant, la différence entre les deux groupes n’était pas statistiquement significative ( p = 0,224).
Conclusion
Les résultats suggèrent que l’augmentation de la force musculaire après entraînement isométrique couplé à du BEMG n’est pas liée au sexe chez les patients arthrosiques.
1
English version
1.1
Introduction
Osteoarthritis (OA) is the most common musculoskeletal condition affecting the quality of life in older adults . A recent survey in India reported the prevalence of OA in older age more than 65 years was 32.6% in rural and 60.3% in urban population . A recent World Health Organization report on the global burden of disease indicates that knee OA is likely to become the fourth most important global cause of disability in women and the eighth most important in men . The major physical impairments such as knee pain, stiffness and decreased quadriceps strength have been associated with knee OA and are believed to contribute to physical disability and progression of the disease . Both radiographic and symptomatic knee OAs are more common among women than men in the age group above 50 years .
Three basic types of therapeutic exercise exist: isotonic, isokinetic, and isometric. Of these three, isometric exercise might be the most appropriate for home maintenance because it requires no or minimal apparatus and it is easy to learn. Further, isometric exercise causes the least intra-articular inflammation, pressure, and bone destruction . Norden et al. acknowledge that “isometric exercises” are simple and inexpensive to perform, and they rapidly improve strength .
The use of EMG-biofeedback (EMG-BF) as an adjunct therapy to standard exercise regime for increasing muscle strength has been investigated in several studies. Adamovich et al. studied the effects of EMG-BF on static contraction of quadriceps muscles. The experimental group, which received auditory and visual EMG-feedback while exercising, demonstrated significantly greater strength gains than the control group, which received no form of feedback. Similarly, Anwer et al. , Lucca et al. , and Khalil et al. found that isometric exercise coupled with EMG-BF lead to significantly greater gains in strength than did isometric exercise alone.
To date, few studies have examined the effect of age and gender on the strength response to strength training (ST). Lemmer et al. examined the effects of age and gender on the strength response to strength training and detraining. They reported that changes in one repetition maximum (1 RM) strength in response to both ST and detraining are affected by age. However, ST-induced increases in muscular strength, appears to be maintained equally well in young and older men and women during 12 weeks of detraining and are maintained above baseline levels even after 31 weeks of detraining in young men, young women, and older men.
Hakkinen et al. investigated the effect of 12-week progressive heavy resistance strength training on electromyographic activity (EMG), muscle cross-sectional area (CSA) of the quadriceps femoris and maximal concentric force in 1 RM test of the knee extensor muscles. Their findings suggested both elderly men and women showed greater increase in maximal dynamic strength accompanied by considerable neural adaptations and muscular hypertrophy.
In a study, Ivey et al. compared (young men, young women, older men and older women) the influence of age and gender on strength and muscle quality response of quadriceps to ST and detraining. All groups demonstrated significant increase in 1 RM strength and muscle volume after training (all P < .05). All groups also increased their maximal force production per unit of muscle mass (Muscle Quality, MQ) with training (all P < .01), but the gain in MQ was significantly greater in young women than in the other three groups ( P < .05). After 31 weeks of detraining, MQ values elevated significantly above baseline levels in all groups ( P < .05), except the older women.
To date however, no study has evaluated the effect of gender on strength gains after isometric exercise coupled with EMG-BF in knee osteoarthritis. So the present study was intended to evaluate the effect of gender on strength gains after isometric exercise coupled with EMG-BF in knee osteoarthritis. We hypothesized that the male group may gain greater strength after training as compare to female group. This study would be helpful for designing strength training protocol for male and female in these populations. If our hypothesis proved that male group gains greater strength after this training as compare to female group, then we have to consider gender differences during formulation of such training protocol. However, if both groups would show similar gains in muscle strength, we can design similar training protocol for both males and females.
1.1.1
Methods and materials
1.1.1.1
Study design
This was a pretest posttest experimental group designed to evaluate the effect of gender on strength gains after five week training programme that consisted of isometric exercise coupled with EMG-BF to the quadriceps muscle in patients with knee osteoarthritis. The subjects were screened first according to the inclusion and exclusion criteria. The subjects were then divided into two groups based on their gender. The study has approval by Institutional Ethical Committee (IEC) and written consent was obtained from all the participants.
1.1.1.2
Subjects
The criteria for inclusion were: radiological evidence of primary osteoarthritis with grade 2 on the Kellgren Lawrence scale, age between 40–65 years; unilateral or bilateral involvement (in case of bilateral involvement the more symptomatic knee was included); pain in and around knee. Subjects were excluded if they had any deformity of the knee (fix flexion deformity), hip or back, any central or peripheral nervous system involvement, received steroids or intra-articular injection within previous three months, uncooperative patients and those who received physiotherapy treatment in the past six months.
Due to a lack of knowledge of previous effect size, sample size calculation was performed based on test results of the change in isometric quadriceps strength, including the first 10 patients (five patients in each group) of the present study. On the basis of results of pilot study, we estimate that male group would gain 45% greater strength as compare to female group. The standard deviation was found to be 1.50. A significance criterion of .05 and power of 0.80 yields a sample size of n 43.74. Therefore, a total of 44 patients (rounding n to the nearest even number) should be enrolled in the study. The following equation was used to calculate the sample size .
n = 4 σ 2 z crit + z pwr 2 D 2
1.1.2
Intervention
Both the groups performed isometric exercises coupled with EMG-BF for five days a week for five weeks.
1.1.2.1
Biofeedback training
Biofeedback training was performed with a Myomed 932 (Enraf Nonius, Rotterdam, The Netherlands), a two-channel EMG machine. Clear and full screen displayed the EMG signal with a curve was obtained for both the vastus medialis oblique (VMO) and rectus femoris (RF).
1.1.2.2
Electrode placement
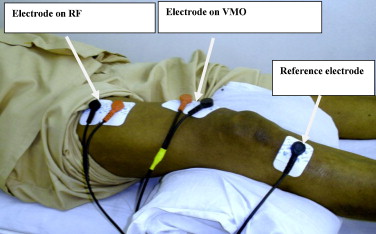
Before the electrode placement, the subjects were asked to shave the part (as required) and then the part to be treated was thoroughly washed by alcohol solution to clean the area and to reduce the skin resistance. Skin adhesive surface electrodes were used to record muscle activity. Two electrodes were placed 4 cm superior and 3 cm medial to supero-medial border of patella, to record the recruitment of VMO. Other electrodes were placed at the junction of the middle and lower third of the thigh, slightly medially and angled downwards (i.e. midway between a line drawn between the base of patella and the anterior superior iliac spine) for rectus femoris. The two active electrodes from each channel were placed as close together as possible along the directions of the fibers of each muscle. The reference electrode was placed below the tibial tubercle ( Fig. 1 ).
Related posts:
 Video illustration in scientific journals and its interest in physical and rehabilitation medicine
Aerobic capacities and exercise tolerance in neuromuscular diseases: A descriptive study
Video illustration in scientific journals and its interest in physical and rehabilitation medicine
Aerobic capacities and exercise tolerance in neuromuscular diseases: A descriptive study
 Care related pain and functional restoration for chronic low back pain: A prospective study
Care related pain and functional restoration for chronic low back pain: A prospective study
 Evolution of life expectancy of patients with Duchenne muscular dystrophy at AFM Yolaine de Kepper centre between 1981 and 2011
Evolution of life expectancy of patients with Duchenne muscular dystrophy at AFM Yolaine de Kepper centre between 1981 and 2011
 Job satisfaction evaluation in low back pain: A literature review and tools appraisal
An unusual cause of foot clonus: Spasticity of fibularis longus muscle
Job satisfaction evaluation in low back pain: A literature review and tools appraisal
An unusual cause of foot clonus: Spasticity of fibularis longus muscle
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


