Distraction-Based Growing Rods— Including Hybrids
Daniel J. Miller
Michael G. Vitale
INTRODUCTION
Early-onset scoliosis (EOS) is characterized by spinal deformity present before 10 years of age. EOS has a variety of etiologies including congenital, syndromic, neuromuscular, and idiopathic. When compared to adolescent idiopathic scoliosis, EOS is associated with numerous comorbid conditions and with increased mortality (1).
EOS is classified according to Classification of Early-Onset Scoliosis (C-EOS) criteria as described by Williams et al. (2) The C-EOS takes into account curve etiology, severity, sagittal plane, and an optional modifier for recent curve progression.
Management options for EOS include observation, bracing, casting, and surgical modalities. While evidence supports the use of casting and bracing in the management of idiopathic EOS before the curve progresses too far, the success of these nonoperative modalities has been limited in the syndromic, neuromuscular, or congenital population.
Surgical options for EOS are divided into distraction-based constructs, compression-based constructs, guided growth systems, and spinal fusion (3). While little consensus exists among experts regarding the optimal choice of surgical intervention, spinal fusion is generally avoided in this young population given the poor outcomes associated with thoracic insufficiency syndrome (4).
Distraction-based systems correct and control spinal deformity through application of distracting forces directly or indirectly to the spine. This can be achieved with traditional growing rod constructs or hybrid growing rod constructs or with the vertical expandable prosthetic titanium rib (VEPTR). The VEPTR was originally developed for the treatment of thoracic insufficiency syndrome and involves distraction indirectly applied to the spine anchors on the ribs. Use of the VEPTR device is discussed elsewhere in this textbook and will not be addressed in this chapter.
In this chapter, we describe the principles involved in treating EOS with distraction-based growing rods and hybrid instrumentation. Traditional growing rod constructs involve limited posterior spinal instrumentation and fusion at cephalad and caudal levels with intervening rod(s) (Fig. 41-1) (5). As the patient grows, the intervening rods are periodically lengthened with the goal of maintaining deformity correction while stimulating growth of the spine and thoracic cage. Hybrid constructs combine elements of both traditional growing rod and concepts popularized with VEPTR and may include connections between the spine and rib (Fig. 41-2), rib and pelvis (Fig. 41-3), or spine and pelvis.
INDICATIONS/CONTRAINDICATIONS
Indications for growing rods are developing and not literature based at this time. As early spinal fusion is associated with poor pulmonary outcome, some type of growth friendly implant is generally favored over early fusion. Indications for growing surgical instrumentation include severe
and/or progressive spinal deformity in a patient who has significant growth remaining and either who is not a candidate for nonoperative management or in whom nonoperative management has failed. Often, these curves are greater than 50 degrees and/or are progressing rapidly (≥10 degrees per month) between examinations.
and/or progressive spinal deformity in a patient who has significant growth remaining and either who is not a candidate for nonoperative management or in whom nonoperative management has failed. Often, these curves are greater than 50 degrees and/or are progressing rapidly (≥10 degrees per month) between examinations.
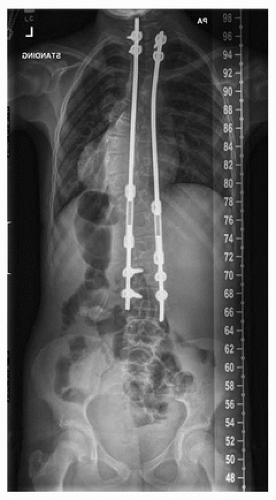 FIGURE 41-1 An anteroposterior radiograph demonstrating pedicle screw fixation at proximal and distal foundations. |
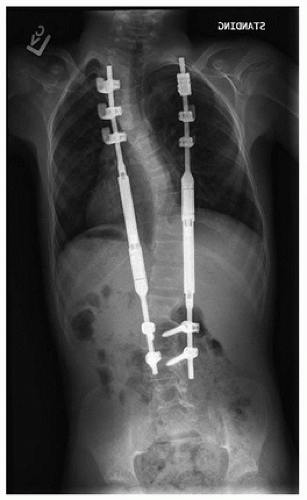 FIGURE 41-2 An anteroposterior radiograph demonstrating rib hook fixation proximally and pedicle screw fixation distally. |
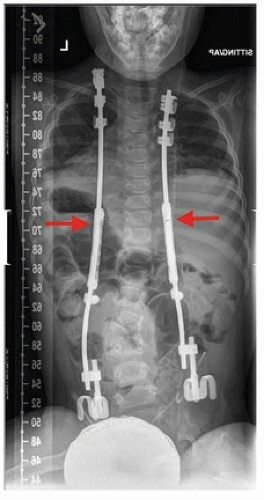 FIGURE 41-3 An anteroposterior radiograph demonstrating rib hook fixation proximally and pelvic saddle fixation distally. The red arrows demonstrate an intentional space between the rods within the growing rod connector so one can see on radiographs that lengthening must take place at the lower end of the connector. |
Contraindications to surgical intervention include patients deemed medically unable to undergo the planned procedure with reasonable safety, patients with active infection or soft-tissue compromise, patient with insufficient bone stock or anatomic variants that preclude safe instrumentation, or patients/caregivers who are unable to maintain appropriate clinical follow-up.
PREOPERATIVE PREPARATION
Preoperative preparation includes history and physical with a multisystem review of systems. A multidisciplinary medical evaluation is essential for preoperative medical optimization and may begin with evaluation by the patient’s pediatrician. The utility of additional specialist consultation will vary based on the comorbid conditions of the patient but may include cardiology, pulmonology, neurology, or gastrointestinal evaluation. Plastic surgery consultation may be considered in patients with anticipated wound healing difficulty. Nutrition is recognized to be a critical factor in wound healing and should be optimized preoperatively. However, growing rods aid children in improving their nutritional status, so poor nutritional status is not a contraindication to growing rods and is commonly present in these sickly children. Soft-tissue coverage should be carefully evaluated during physical evaluation, and serum laboratory makers including total lymphocyte count, albumin level, prealbumin level, and transferrin level can serve as objective measures of nutritional status. Chlorhexidine wipes may be provided for application the night prior to surgery to decrease bacterial colonization.
Full-length posterior-anterior and lateral views should be obtained for preoperative planning. Preoperative side bending, supine, and traction films can help to determine curve flexibility and plan correction strategies. Advanced imaging with magnetic resonance imaging (MRI) is recommended to evaluate for neuraxial abnormality, which has an increased incidence in the EOS population. Radiographs and advanced imaging should be evaluated closely for evidence of congenital osseous abnormalities including occult spina bifida.
Multiple options for anchor and rod constructs are available, and previous studies have demonstrated high variability among surgeons (6). Factors that influence choice of construct include patient size, habitus, osseous anatomy, sagittal profile, muscle tone, ambulatory capacity, bone quality, and surgeon preference. Traditional growing rod and hybrid constructs are lengthened via small open surgical procedures, whereas newly approved devices are lengthened by application of an
externally controlled, magnetic device in an outpatient setting (7). Externally controlled lengthening has the theoretical benefit of fewer complications related to open surgical procedures including infection, wound problems, and medical and psychosocial issues related to general anesthesia.
externally controlled, magnetic device in an outpatient setting (7). Externally controlled lengthening has the theoretical benefit of fewer complications related to open surgical procedures including infection, wound problems, and medical and psychosocial issues related to general anesthesia.
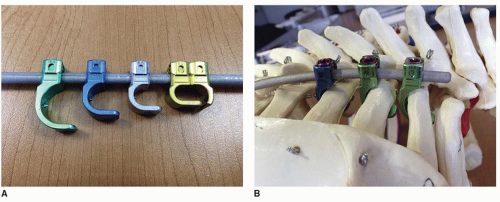 FIGURE 41-4 A. Example of various hooks that can be used as spine anchors. B. Example of hooks positioned as spine anchor in a distraction-based construct. (Used with permission of the Children’s Orthopedic Center, Los Angeles, CA.) |
In planning sites of cephalad and caudal foundations for growing rods, each site must be capable of withstanding distractive forces over a prolonged period without mechanical failure or loosening. The upper foundation is usually at the T2-T4 levels, whereas distal foundation level is most frequently at the L2-L3 levels. Pelvic instrumentation may be utilized as an alternative distal foundation levels, particularly in neuromuscular patients with significant pelvic obliquity (e.g., greater than 15 degrees) (8). A rule of thumb is not to put growing rods any further caudal than you would plan on doing a final fusion and avoid going to the pelvis in ambulators if the deformity can be controlled without pelvic fixation.
Dual growing rod constructs have been shown to provide improved initial deformity correction and are associated with fewer complications when compared to single rod constructs (9). As such, dual rod constructs should be utilized if at all possible provided that patient habitus and soft-tissue envelope accommodate.
In terms of upper anchors, pedicle screws are strong, but can be challenging to place and can pull out into the spinal canal causing paralysis, particularly if there are less than four to six pedicle screws with good purchase. In such cases, the rod may break before the pedicle screws pull out, particularly if a smaller (4.5 to 4.75 mm) rod is used. Pedicle screws and spine hooks are generally considered to lead to a local fusion. An advantage of spine and rib hooks is they tend to fail in a posterior direction, which does not place the spinal cord at risk. Traditional spine hooks, or specialized hooks, may be used as anchors on the ribs (Fig. 41-4A, B). Additional advantages of rib anchors are that (a) ribs tend to provide good purchase with reasonable bone quality even in an osteopenic child with poor-quality bone in the spine, (b) they are in a valley between the scapula and spinous process so soft-tissue coverage is often better than spine anchors, (c) there may be some protection against rod breakage and PJK compared to spine anchors, and (d) there is no dissection or intentional fusion of the proximal spine. Our current practice is to use multiple rib anchors (e.g., ≥4) when implanting growing rod constructs in children under 8 years of age in order to distribute load.
SURGICAL PROCEDURE
After induction of general anesthesia and initiation of neuromonitoring of both upper and lower extremities, the patient is positioned prone on an OSI Jackson tabletop with careful attention to bony prominences.
Preoperative antibiotics are administered within 1 hour of incision. A first-generation cephalosporin (e.g., cefazolin) as well as an aminoglycoside (e.g., tobramycin) is routinely used for prophylaxis against common skin flora; vancomycin may be used instead in the setting of allergy or known history of methicillin-resistant Staphylococcus aureus (MRSA). A patient safety checklist (Fig. 41-5




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
