Fractures
M. Bradford Henley
Michael J. Gardner
Sterile Instruments/Equipment
- Extra Mayo stand cover or adhesive bag as fluid collection drape
- Impervious stockinette and 4 inch elastic bandage wrap for forearm and hand
- Bipolar cautery for ulnar neurolysis dissection, if required
- 1/4% Marcaine with epinephrine for posterior arm skin and subcutaneous tissues prior to incision
- Tourniquet if desired
- Large and small pointed bone reduction clamps (“Weber clamps”)
- If planning proximal ulnar osteotomy: micro oscillating saw, small osteotomes (e.g., Hooke osteotomes)
- Implants:
- Anatomically contoured periarticular plates for application to the medial and lateral humeral columns, 2.7/3.5 reconstruction plates, 3.5 compression plates
- Consider cannulated 3.5- or 4.0-mm screw(s) for stabilizing the intercondylar split.
- Consider small and mini-fragment screws and mini-fragment plates (2.0/2.4 mm) if comminuted medial and/or lateral columns.
- Anatomically contoured periarticular plates for application to the medial and lateral humeral columns, 2.7/3.5 reconstruction plates, 3.5 compression plates
- K-wires and wire driver/drill
Patient Positioning
- Position the patient either prone or lateral.
- Radiolucent table extension; cantilever-type.
- Patient is placed backwards so that the patient’s head is toward the radiolucent and “foot end” of the table.
- U-drape to exclude the axilla and thorax.
- If prone, support fractured arm by radiolucent (e.g., Plexiglas) board placed orthogonally to table so that board is supported by patient’s torso and weight; Plexiglas board is placed under table’s “mattress pad.”
- Most arm tables are too long and do not permit sufficient elbow flexion when patient is prone.
- Center Plexiglas on patient’s shoulder so that arm is abducted at a right angle to torso; this aids in obtaining lateral images.
- Most arm tables are too long and do not permit sufficient elbow flexion when patient is prone.
- If positioned laterally, an elevated arm board that can be adjusted for height is needed.
- In either position, the contralateral arm is supported by an arm board designed for prone positioning, so excessive abduction and external rotation are avoided.
- Radiolucent table extension; cantilever-type.
- OR table is rotated 90 degrees with respect to usual position in room, to provide unimpeded access to shoulder, arm, and elbow.
- C-arm is positioned above patient’s head, parallel to long axis of patient’s body and perpendicular to the injured extremity which is abducted 90 degrees. This permits AP and lateral imaging without moving the extremity (Figs. 6-1 and 6-2).
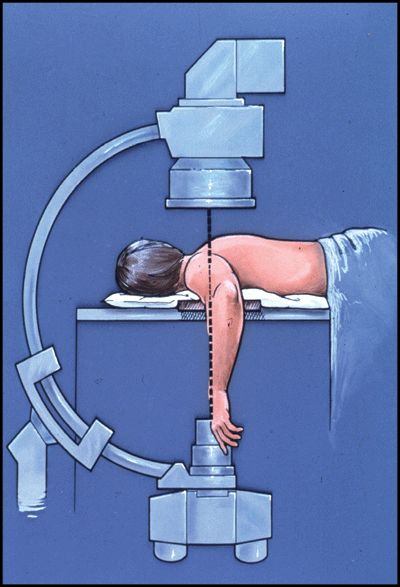
Figure 6-1. Prone positioning with arm supported by radiolucent Plexiglas board allows for unimpeded AP and lateral images from shoulder to elbow. The contralateral upper extremity may be positioned at the patient’s side or abducted comfortably. Also, it is not near the operative field being imaged with X-ray.

Figure 6-2. In the lateral position, the contralateral upper extremity may impede some AP images. This can be avoided by carefully positioning the contralateral extremity and by canting the C-arm anode toward the patient’s torso. After draping, the forearm and hand of the injured extremity are placed in an impervious stockinette and over wrapped with an elastic bandage to reduce dependent edema. The extremity is contained in a second Mayo stand cover which is used to collect irrigation fluid and to keep the operative field tidy. A fenestration is made in the dependent end of the Mayo stand cover; it is weighted with a clamp and placed in a kick bucket as a fluid collection reservoir.
Surgical Approaches
- Place hand and forearm in impervious stockinette, over wrap with ACE.
- Take extra Mayo stand cover and create fenestration at the closed end.
- Attach weighted clamp (e.g., Ochsner/Kocher) at this fenestration (to keep it open and dependent).
- Place this dependent portion of the Mayo stand cover, with clamp, into a kick bucket to collect irrigation fluids.
- Place extremity in normal opening of Mayo stand cover (Fig. 6-2).
- Alternatively, use commercially available, triangular, irrigation fluid collecting drape.
- Take extra Mayo stand cover and create fenestration at the closed end.
- Posterior midline incision skirting the radial side of the olecranon (Fig. 6-3).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


