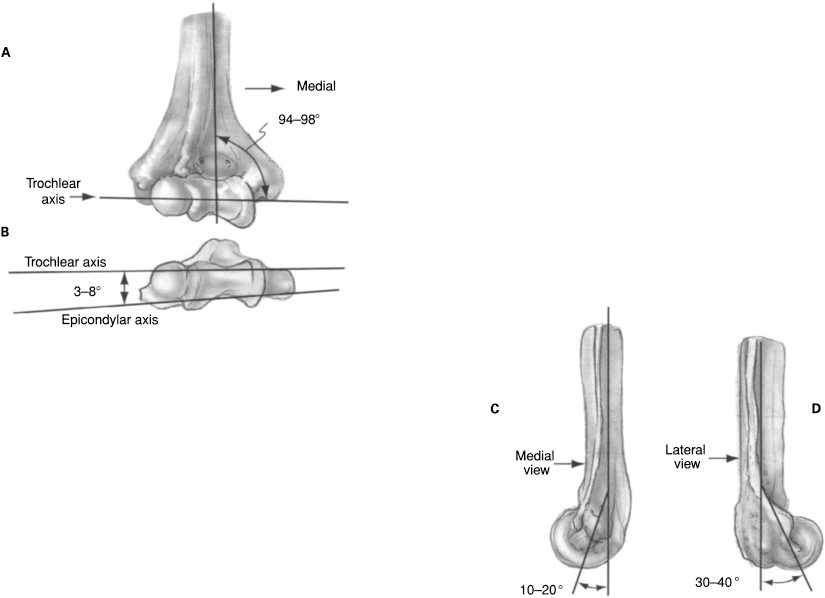
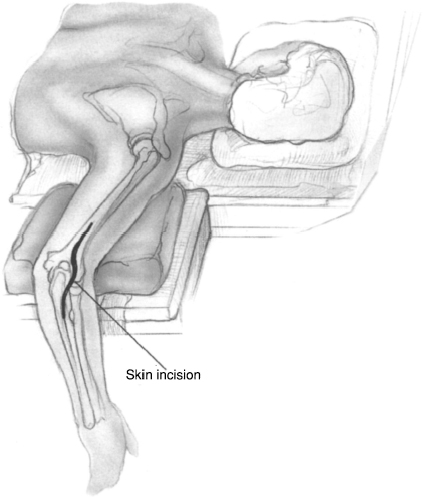
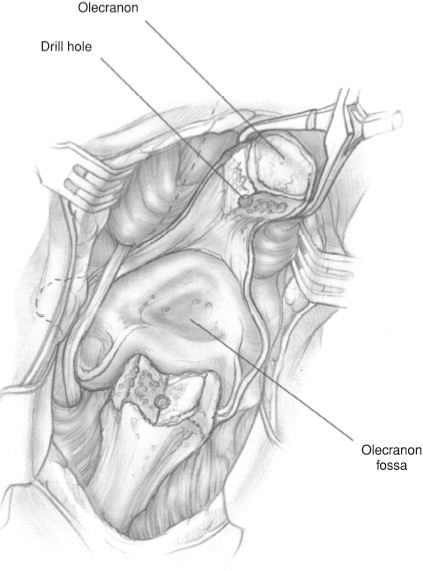
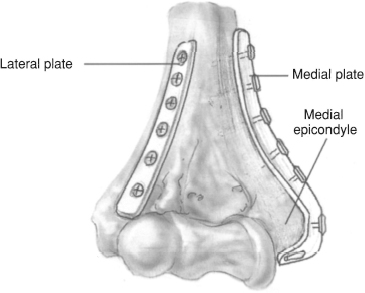
CHAPTER 10 Brian J. Hartigan 1. Intra-articular fracture 2. Unstable nonarticular fracture 3. Associated vascular injury requiring repair 1. Open fracture with contaminated wound 2. Inadequate soft tissue coverage 3. High-operative risk (relative) 4. Severe osteoporosis or comminution (relative) 1. Evaluate patient for other injuries. 2. Assess for open wounds. 3. Document complete neurologic and vascular examination. a. If vascular compromise, perform closed reduction and reassess. If continued vascular compromise, plan for operative exploration and vascular repair/bypass in addition to skeletal stabilization. 4. Obtain adequate radiographs. a. AP and lateral of elbow b. Consider AP and lateral with longitudinal traction. c. Consider radiographs of contralateral extremity for preoperative planning purposes. d. Consider CT scan, especially for intra-articular comminuted fractures. 5. Splint elbow at 90 degrees flexion and ice/elevate until definitive operative fixation. 6. Understand normal elbow anatomy (Fig. 10–1) a. Lateral column diverges approximately 20 degrees from sagittal axis and projects 30 to 40 degrees anteriorly, ending at the capitellar articular surface (Fig. 10–1D). b. Medial column diverges approximately 45 degrees from sagittal axis and projects 10 to 20 degrees anteriorly, ending proximal to the trochlea (Fig. 10–1C). c. Olecranon fossa and coronoid fossa lie between lateral and medial columns and proximal to the trochlea. d. Trochlea internally rotated 3 to 8 degrees and has valgus inclination of 94 to 98 degrees (Figs. 10–1A and 1B). e. Diameter of trochlear sulcus is much smaller than that of the medial trochlear ridge and the lateral condyle. 7. Create operative plan for exposure, reduction and fixation. 8. Consider the need for bone graft. Figure 10–1 (A) Normal elbow anatomy. Trochlea has valgus inclination of 94 to 98 degrees. (B) Normal elbow anatomy.Trochlea internally rotated 3 to 8 degrees. (C) Normal elbow anatomy. Medial column projects 10 to 20 degrees anteriorly, ending proximal to the trochlea. (D) Normal elbow anatomy. Lateral column projects 30 to 40 degrees anteriorly, ending at the capitellar articular surface Figure 10–2 Patient position. The patient is placed in a prone position with the arm on a short armboard and the elbow flexed. Figure 10–4 Olecranon osteotomy. The tip of the olecranon and the attached triceps tendon are reflected proximally to visualize the distal humerus. Figure 10–5 Reconstruction plates.The medial and lateral columns are fixed to the humeral shaft using medial and posterolateral reconstruction plates. 1. Patient is positioned in a prone position with the arm on a short armboard and the elbow flexed or in a lateral decubitus position with the involved arm draped over a bolster (Fig. 10–2).
Distal Humeral Fractures
Indications
Contraindications
Preoperative Preparation
Special Instruments, Position, and Anesthesia
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


