Distal Femoral Osteotomy for Crouch Gait
Tom F. Novacheck
DEFINITION
Crouch gait is defined as walking with excessive knee flexion during stance.
Crouch is a common walking pattern in neuromuscular conditions, particularly for individuals with cerebral palsy.
Many potential abnormalities of bone alignment and joint flexibility can accompany or lead to crouch gait.
Persistent crouch in adolescence frequently results in fixed knee flexion deformity and patella alta.
Potential contributing factors include hamstring contracture, hip flexion deformity, foot deformity, loss of plantarflexion-knee extension couple, excessive femoral anteversion, and external tibial torsion. Weakness and impaired motor control are contributing factors. For some patients, disorders of balance or sensory impairments are major contributors.1
Fixed knee flexion deformity is oftentimes associated with patella alta. Fixed knee contracture and patella alta are the components of the pathology that are treated with these procedures.
ANATOMY
Typical knee extension range is 0 degrees (full knee extension).
Posterior capsular contracture can result from the imbalance between spastic or contracted hamstrings and knee extensor dysfunction (often associated with patella alta).
Distal femoral anatomy is normal, although torsional deformity (excessive femoral anteversion) is commonly seen in neuromuscular conditions, especially cerebral palsy.
PATHOGENESIS
The pathogenesis of knee flexion deformity and crouch gait in cerebral palsy will be described, as it is the most common condition to be treated with this technique. However, other causes of knee flexion deformity and persistent crouch could be treated similarly.
Preterm, perinatal, or infantile brain injury leads to static encephalopathy.
This neurologic disorder causes hypertonia (commonly spasticity), impaired motor control, and weakness.
Typical muscle growth results from the tension produced by normal bone growth and age-appropriate, typical gross and fine motor activities.
Musculotendinous growth in children with cerebral palsy is delayed because spastic muscle does not grow normally in response to stretch and delays in attainment of typical functional activities.
Bone growth and joint development are also adversely affected by a lack of normal functional activities as well as spasticity and musculotendinous contracture.
NATURAL HISTORY
Crouch gait is not uncommon at 5 to 7 years of age. At these ages, the primary causes are spasticity, weakness, and impaired balance mechanisms.
If crouch persists during later childhood, musculotendinous contractures of the two-joint muscles (psoas, hamstrings, rectus femoris, and gastrocnemius) develop. Persistent alignment in a crouch position leads to excessive elongation of the one-joint muscles (gluteus maximus, quadriceps, and soleus), which are primarily responsible for normal upright posture.1
The soleus, in particular, is responsible for restraining the forward movement of the tibia over the plantigrade foot (also known as the plantarflexion-knee extension couple).1 As a result, the ground reaction force vector typically falls near the knee joint in midstance, minimizing the demand on the quadriceps to maintain knee extension.
If weak or elongated, the ankle plantarflexors are no longer able to restrain the forward movement of the tibia over the plantigrade foot (loss of the normal plantarflexion-knee extension couple).
Further growth leads to loss of knee joint mobility and the development of posterior capsular contracture.
For some patients in adolescence, pain from stress fractures or from excessive stress in the patellofemoral joint itself can lead to a precipitous worsening of crouch.
Knee pain, decreased ambulatory function, or the loss of walking ability in adulthood in individuals with cerebral palsy is common.3
PATIENT HISTORY AND PHYSICAL FINDINGS
Physical examination methods include the following:
Knee range of motion: Loss of extension indicates a posterior capsular contracture; loss of flexion could be due to quadriceps contracture and especially rectus femoris spasticity or contracture if the knee is flexed in the prone position. Normal upright walking requires full knee extension range of motion.
The examiner should palpate the inferior pole of the patella and tibial tubercle. This distance is typically equal to patellar length. The patella is pushed medial to lateral to detect patellar instability. Patella alta, which can be a cause of knee pain or can contribute to knee extensor dysfunction, is suspected if
The distance from the inferior pole of the patella to the tibial tubercle exceeds patellar height.
The patella is unstable medial to lateral.
The patellar tendon (as opposed to the patella) lies in the patellofemoral groove.
With the knees in extension, the superior pole of the patella is typically one fingerbreadth proximal to the adductor tubercle.
Knee extension lag test: Normal extension lag is 0 degree. Terminal knee extension strength is required to control knee flexion during loading response.
Hamstring contracture: Normal popliteal angle can be as much as 30 degrees during preadolescence. It is commonly greater in boys than in girls. For differential diagnosis purposes, it is important to identify all potential contributors to crouch gait.
If resistance is felt as the popliteal angle is being assessed, hamstring spasticity is identified. If the knee is flexed with the patient prone and the hip extended, spasticity of the rectus femoris is identified.
Spasticity is one of the primary causes of the series of events that ultimately leads to crouch. If severe enough, direct spasticity treatment may be necessary.
A complete examination of the patient should also include evaluation of associated abnormalities to identify all potential contributors to crouch gait, including hip flexion deformity, hamstring contracture, femoral anteversion, tibial torsion, foot deformity or instability, balance disorder, and visual or sensory disturbances.
IMAGING AND OTHER DIAGNOSTIC STUDIES
A plain lateral radiograph of the knee in maximum extension should be obtained to assess for fixed knee flexion contracture and patella alta (FIG 1).
If the knee is held in maximum extension, the femoral-tibial angle on the lateral radiograph represents the degree of true knee flexion deformity.
The knee is extended maximally with a bolster just below the patella to assess the true degree of patella alta. Patella alta can be documented using the Insall ratio or the Koshino index.2
Inferior pole sleeve avulsion injuries of the patella are common in children with spastic cerebral palsy and can be identified on the lateral radiograph. The development of a stress fracture is typically painful and can lead to the rapid progression of crouch over a short period.
Computerized gait analysis provides much needed insight to create a problem list to guide treatment decision making by identifying the numerous other contributors to crouch gait listed earlier.
DIFFERENTIAL DIAGNOSIS
Knee extensor lag with or without patella alta
Hamstring spasticity or contracture
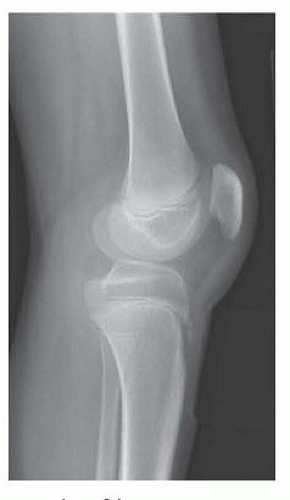
FIG 1 • Lateral radiograph of knee in maximum extension. Patellar position and degree of knee contracture can be assessed from this view.
Hip flexor spasticity or contracture
Femoral anteversion
Tibial torsion (typically external)
Ankle plantarflexor insufficiency
Foot deformity
Excessive midfoot instability
Soleus weakness: primary versus iatrogenic from prior Achilles tendon lengthening
NONOPERATIVE MANAGEMENT
Physical therapy (stretching and strengthening) helps minimize the development of musculotendinous contracture secondary to spasticity and weakness.
Botulinum toxin injections or oral spasmolytic agents can help manage spasticity.
Functional strengthening of the muscle groups that contribute to crouch (ankle plantarflexors, knee extensors, and hip extensors) can help correct muscle imbalance.
Nighttime knee extension splinting with knee immobilizers or bivalved casts can help prevent a flexed knee position during the night, thereby minimizing the development of knee capsular contracture.
SURGICAL MANAGEMENT
Preoperative Planning
The lateral radiograph of the knee in maximum extension should be reviewed for the degree of knee contracture, patellar height, presence of a stress fracture at the inferior pole of the patella, and the status of skeletal maturation (see FIG 1).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








