Direct Anterior Approach for Hip Arthroplasty
Patient Selection
Indications
Primary total hip arthroplasty (THA)
Hemiarthroplasty for femoral neck fractures
Relative Contraindications
Patients who have obesity or are muscular
Patients with short varus femoral necks
Dysplasia or deformity
Revision THA
Preoperative Imaging
AP pelvis
AP hip
Cross-table lateral hip
Procedure
Room Setup/Patient Positioning
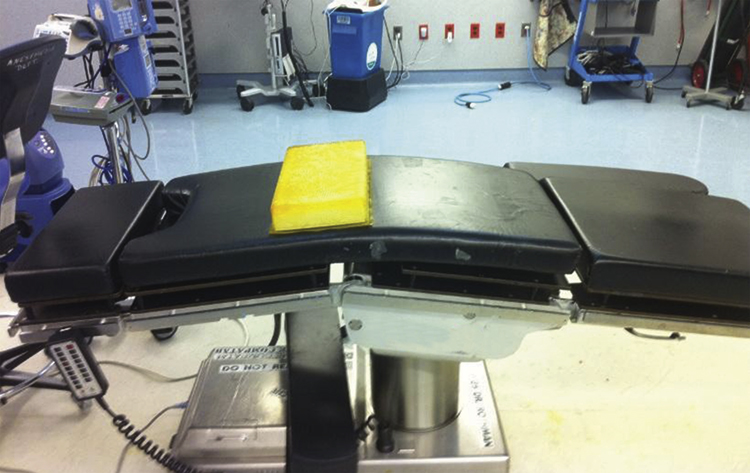
Figure 1Photograph shows the room setup using a standard operating table for the direct anterior approach for total hip arthroplasty. The gel bump, 30° of table flexion, and the distal arm board on the nonsurgical side of the table facilitate the extension and adduction of the surgical lower extremity necessary for femoral exposure.
Standard radiolucent table
Supine position
Hip flexion, adduction, and external rotation of surgical side are required
Flexion—Place bump under pelvis and flex table 30° before femoral preparation (Figure 1)
Adduction—Attach arm board distally on nonsurgical side of table; place nonsurgical leg onto arm board during femoral preparation to clear space on table for surgical extremity
External rotation—Applied gently by second assistant when required
Prepare and drape surgical leg free
Special Instruments
Curved or offset reamers and broaches to facilitate femoral and acetabular preparation
Certain femoral implant design features, such as reduced lateral shoulder and contoured distal tip, facilitate femoral reconstruction
Surgical Technique: Total Hip Arthroplasty
 | Video 57.1 Direct Anterior Approach for Total Hip Arthroplasty. Gregory K. Deirmengian, MD; William J. Hozack, MD (23 min) |
Incision Planning and Superficial Dissection
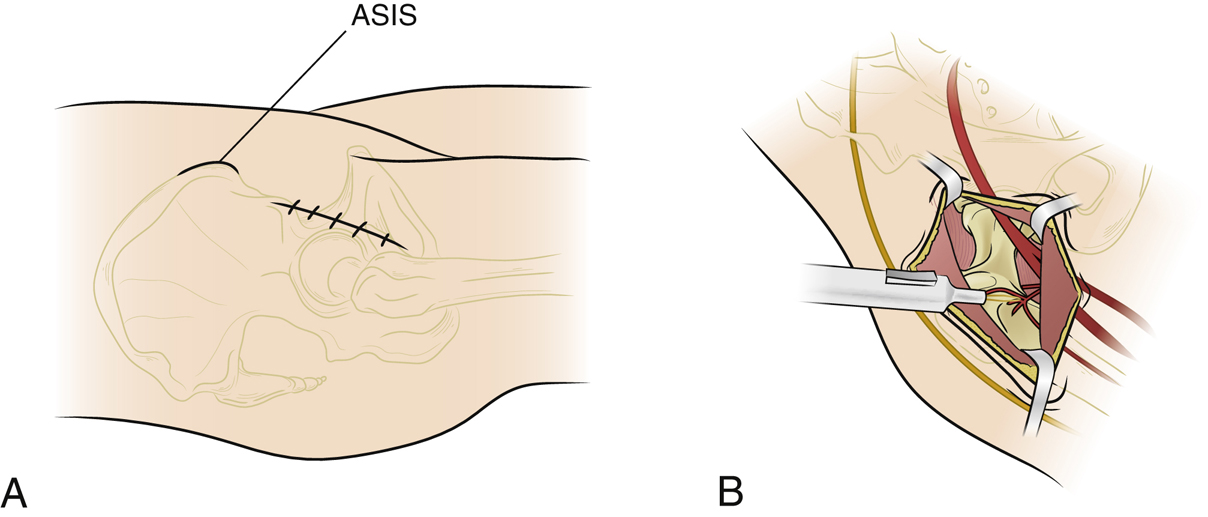
Figure 2Illustrations demonstrate incision planning, dissection, and exposure for total hip arthroplasty using the direct anterior approach. A, The anterior superior iliac spine (ASIS) is marked as a landmark. The marking for the incision starts 2 to 3 cm distal and 2 to 3 cm lateral to the inferomedial corner of the ASIS and proceeds distally 8 to 10 cm with a gentle lateral angle. B, The lateral femoral circumflex vessels and their branches are cauterized.
Careful planning of skin incision is critical
Palpate and mark borders of anterior superior iliac spine
Mark the planned incision 2 to 3 cm distal and 2 to 3 cm lateral to the anterior superior iliac spine
Carry planned incision 8 to 10 cm distal with a gentle lateral slope (Figure 2, A)
If tensor fascia lata (TFL) is palpable, make incision in its midline and follow its course proximally and distally
Sharply incise skin and subcutaneous fat and use electrocautery as needed for coagulation
Incise Scarpa fascia and sweep off deep fascia encasing TFL
Identify the TFL; its medial border is defined by a fat stripe, and its midpoint is defined by small perforating vessels
Divide fascia overlying TFL in the midpoint of TFL; reflect fascia medially to medial border of TFL
Insert finger posteriorly into interval between TFL and sartorius for blunt dissection to the level of anterior capsule
Direct finger posterolaterally to reach space between abductors and capsule
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


