(1)
Department of Orthopedic Surgery Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Abstract
An isolated rupture of the posterior deep part of the deltoid ligament is a rare injury. In case of bony avulsion, most of these lesions heal by fibrous union and pseudarthrosis. In case of a persisting painful posteromedial swelling, CT scan can confirm the avulsion. The avulsion fragment can be successfully removed by means of a two-portal hindfoot approach. The anatomy, trauma mechanism, history and physical examination, therapeutic options, and operative technique for endoscopic treatment by means of a two-portal hindfoot approach are given.
Chronic deltoid ligament pain most often involves the posteromedial deep portion of the deltoid ligament.
In a patient with persisting posteromedial pain and swelling, a CT scan can confirm an avulsion or calcification of the deep portion of the deltoid ligament.
These symptoms can be treated by means of a two-portal hindfoot approach.
16.1 Introduction
Rupture of the deltoid ligament frequently occurs in combination with an ankle fracture such as a pronation exorotation fracture or type 4 supination exorotation fractures (Van den Bekerom et al. 2009; Van den Bekerom and Van Dijk 2010). An isolated rupture of the deltoid ligament is a rare injury. Lauge-Hansen and Ankelbrud (1942) stated that rupture of the deltoid ligament can occur as an isolated injury, caused by pronation and outward rotation (Lauge-Hansen and Ankelbrud 1942).
Broström reported in his material the frequency of isolated deltoid ligament rupture to be 2 % (Broström 1966).
Cedell reported on four cases of an isolated rupture of the deep portion of the deltoid ligament in which a pulled-off bone fragment, consisting of the insertion of the ligament in the talus, was present (Cedell 1974).
16.2 Anatomy
The deep portion of the deltoid ligament runs from the dorsal and distal part of the medial malleolus and inserts to the medial tubercle of the talus (Fig. 16.1). To the medial tubercle of the talus, the flexor retinaculum of the flexor hallucis longus has its insertion as well.
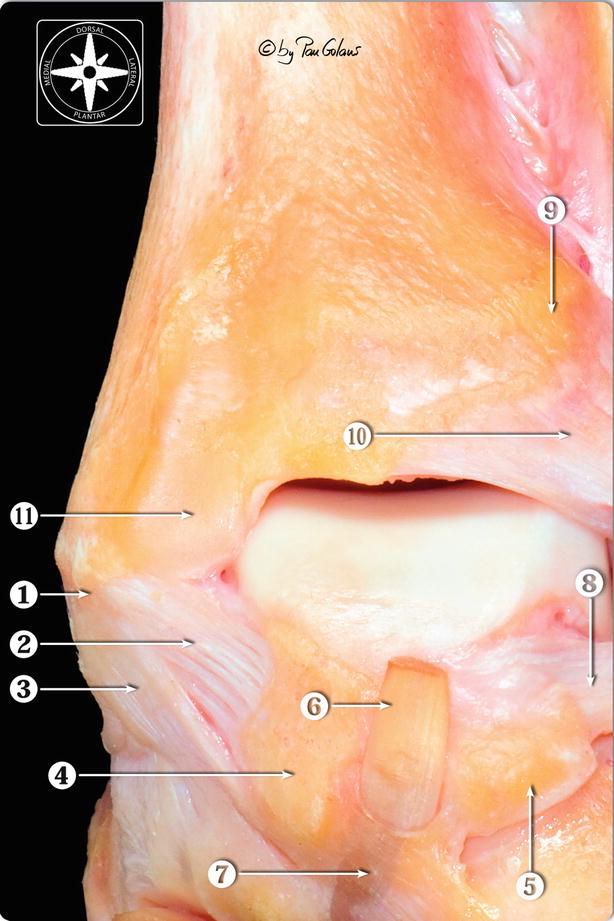
Fig. 16.1
Close-up of the posteromedial area of the osteoarticular dissection of the ankle. The posterior intermalleolar ligament has been resected. 1 Medial malleolus (posterior colliculi). 2 Deep posterior tibiotalar ligament (deep layer of the superficial medial collateral ligament). 3 Tibiocalcaneal ligament (superficial layer of the superficial medial collateral ligament). 4 Medial talar process. 5 Lateral talar process. 6 Flexor digitorum longus tendon (cut). 7 Flexor hallucis longus retinaculum. 8 Posterior talofibular ligament. 9 Posterior tubercle of the tibia. 10 Superficial component of the posterior tibiofibular ligament (With kind permission of © Pau Golanó 2013)
16.3 Trauma Mechanism
The deep portion of the deltoid ligament stabilizes the ankle joint when the talus occupies a position of dorsal extension and pronation in the ankle mortise (Cedell 1974). With a heavy breaking force in the direction of dorsal extension and pronation, the strength of the ligament can be exceeded and a rupture can occur which can be combined with the avulsion of a bone fragment from the talus. Avulsion of the flexor retinaculum can occur in case of a heavy pulling force of the flexor hallucis longus onto the retinaculum.
16.4 History and Physical Examination
After a distortion of the ankle, swelling of the posteromedial joint persists with pain and difficulty in weight bearing. In chronic cases patients are able to walk and run on even ground, but they have difficulties with more demanding exercises like running on uneven ground or making a sudden change of direction. On examination there is a local swelling behind the medial malleolus. This protruding aspect of the posteromedial talus is tender by palpation. Otherwise, the ankle is painless and has a normal range of motion.
X-ray is usually negative. The CT scan will disclose the avulsion fragment (Fig. 16.2a).
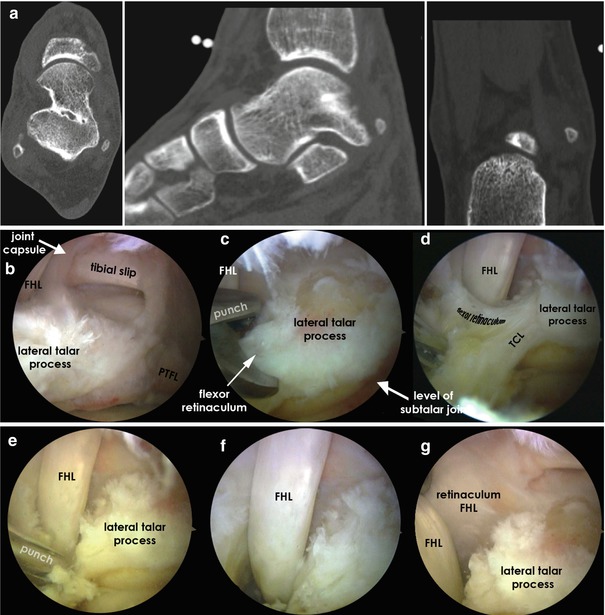
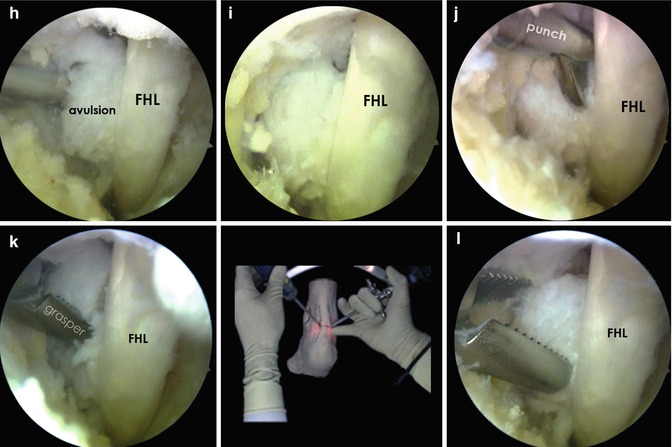
Fig. 16.2




A 32-year-old male patient with posteromedial right ankle pain. Problem started after trauma while playing soccer. Trauma mechanism remains uncertain. Initial treatment with ankle taping for 6 weeks. Since then persisting pain posteromedially. On investigation posteromedial swelling with recognizable tenderness at the level of the tarsal tunnel. No Tinel sign and no irritation of the flexor hallucis longus. No irritation of the posterior tibial tendon. Normal sensation. X-ray: no abnormality. (a) CT scan in three directions shows a calcification medial from the posteromedial talar process. The diagnosis: Cedell fracture. The calcification is an avulsion of the deep portion of the deltoid ligament or an avulsion of the flexor retinaculum. Both attach to the posteromedial talar process. Operative treatment by means of two-portal hindfoot approach. Patient in the prone position. Scope in the posterolateral portal. Instruments in the posteromedial portal. (b) Situation after opening the ankle joint and subtalar joint. The tibial slip and below it the ankle joint are clearly visible. The lateral talar process is in the left and middle of the view and the posterotalofibular ligament (PTFL) runs through the lateral side. On the top left we see the flexor hallucis longus. Their remaining joint capsule is visible behind the flexor hallucis longus. (c) A closer look at the distal part of the flexor hallucis longus and the flexor retinaculum. The posterior talocalcaneal ligament (TCL) is visible as well. Both attach to the posterolateral talar process. The first step is cutting the flexor retinaculum and talocalcaneal ligament (TCL). (c) Cutting the flexor retinaculum. (d, e) Cutting the TCL ligament. (f) Situation after full release. (g) The flexor retinaculum is put aside by means of a probe. The probe is just visible between 9 and 10 o’clock. The remnant of the flexor retinaculum attaching to the lateral talar process is seen at 7 o’clock. The other part of the flexor retinaculum which attaches to the posteromedial talar process has now come into view. This has to be detached at the level of the probe. This can be performed by means of a small fragment periosteal elevator or by means of a punch. (h) The flexor retinaculum has now been removed from the posteromedial talar process, and the flexor hallucis longus has been brought back into its sliding channel. The detached loose fragment (“avulsion”) now comes into view medial from the flexor hallucis longus. (i) The fragment is now clearly visible medial from the flexor tendon. (j) Further release of the fragment by means of the punch. Further detachment from the deltoid ligament, the pseudarthrotic area (area between the fragment and the posteromedial talar process), and the flexor retinaculum takes place by means of the punch and small periosteal elevator. (k, l) The fragment is now loose and removed with a grasper
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
