TABLE 34-1 CAUSES OF DELTOID INJURIES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Although many patients demonstrate an uneventful postoperative course, a few develop complications related to dehiscence of the deltoid repair, which can manifest as a residual defect at the muscle’s origin (Fig. 34-1). Similar but less frequent occurrences have been reported after deltopectoral, deltoid splitting, and axillary surgical approaches for instability, degenerative, and traumatic conditions of the shoulder.25 Factors thought to contribute to this postoperative complication include inadequate surgical repair of the deltoid origin, osteoporotic bone unable to withstand the tension afforded by transosseous sutures, poor tissue quality, overzealous retraction, and patient noncompliance. This outcome is avoidable in most cases, but when it does occur, it is typically associated with considerable morbidity and disability.6,20,25,32,45,46,55,56,64
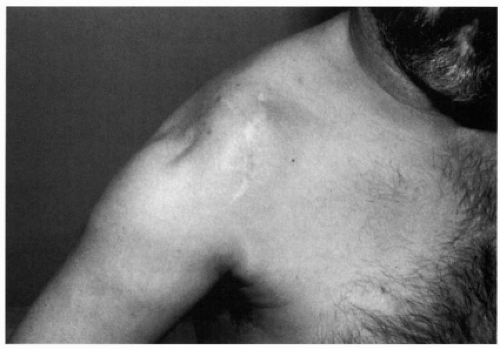 Figure 34-1 Shoulder with middle deltoid detachment 2 years after anterior acromioplasty and rotator cuff repair. |
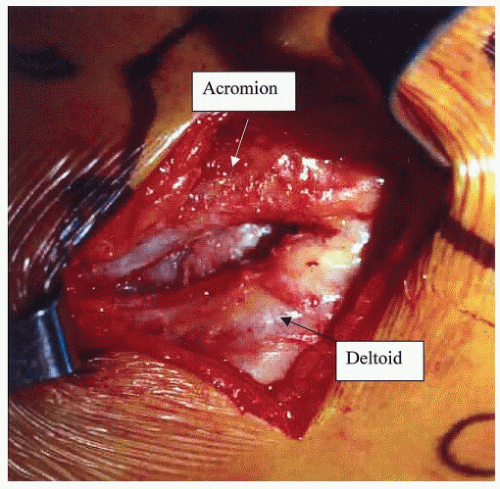 Figure 34-2 Chronic defect in the anterior deltoid origin, seen at the time of revision open repair, secondary to an excessive detachment of the deltoid origin during an arthroscopic acromioplasty. |
resection (acromionectomy), or neurologic impairment in association with deltoid detachment. Pain at the anterolateral aspect of the shoulder, for example, could be related to a refractory rotator cuff disorder, disruption of the deltoid origin, or both. This may also hold true for a patient’s inability to elevate the arm. Evaluation may reveal functional deficits secondary to rotator cuff dysfunction, deltoid dysfunction, or both.
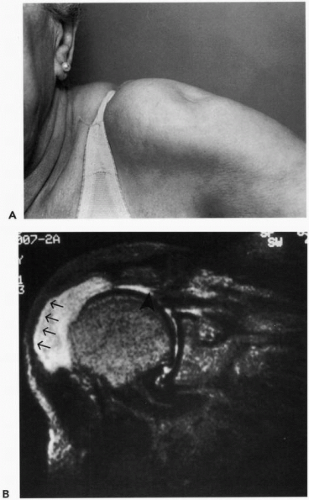 Figure 34-3 (A) Spontaneous middle deltoid origin detachment in a patient with a massive chronic rotator cuff tear. (B) Magnetic resonance scan demonstrates the deltoid origin disruption (arrows) and rotator cuff tear (arrowhead). |
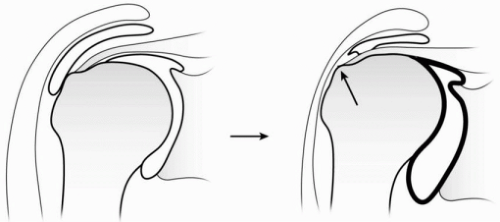 Figure 34-4 Mechanism of wear on the undersurface of the deltoid muscle in a shoulder without (left) and with (right) a rotator cuff tear. A deficient rotator cuff allows for cephalad migration of the humeral head with chronic abrasion of the greater tuberosity against the deltoid muscle. (Reproduced with permission from Morisawa K, Yamashita K, Asami A, et al. Spontaneous rupture of the deltoid associated with massive tearing of the rotator cuff. J Shoulder Elbow Surg 1997;6:556.) |
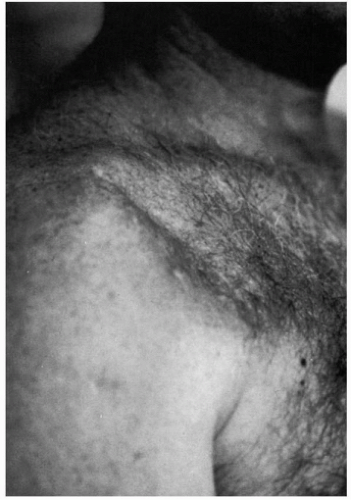 Figure 34-5 Postoperative anterior deltoid detachment. |
the arm at the side, but they can often be appreciated when the humerus is actively abducted. Palpation along the acromion border can facilitate assessment of the size of the defect and the degree of retraction. Frequently, focal tenderness can be elicited at the detachment site. Atrophy of the deltoid or rotator cuff may also be evident and can represent disuse, muscle or tendon injury, or neurologic impairment.
 Figure 34-6 Lateral acromionectomy in a patient with a middle deltoid detachment. |
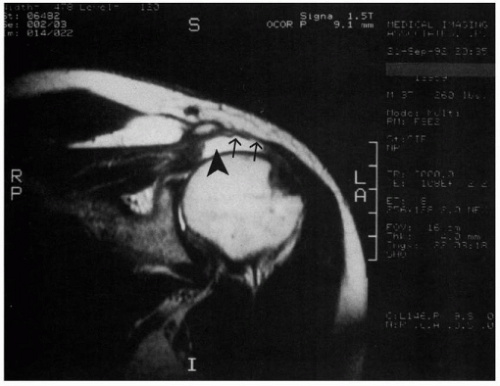 Figure 34-7 Postoperative magnetic resonance image demonstrates a detachment of the middle deltoid (arrows) and full-thickness tear of the supraspinatus tendon (arrowhead).
Related posts: Traumatic Anterior Instability: Arthroscopic Solutions Traumatic Anterior Instability: Arthroscopic Solutions
 Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty? Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
 Acromioclavicular Joint: Difficult Problems and Revision Surgery Acromioclavicular Joint: Difficult Problems and Revision Surgery
 Rotator Cuff Arthropathy: The Unconstrained Arthroplasty Rotator Cuff Arthropathy: The Unconstrained Arthroplasty
 Scapular Winging: Trapezius Dysfunction Scapular Winging: Trapezius Dysfunction
 Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|