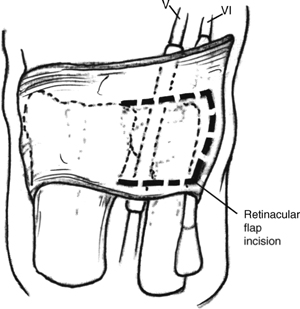
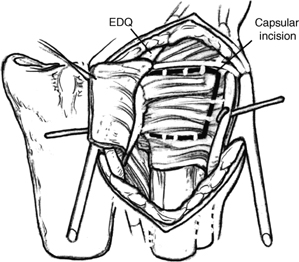
21 Darrach Procedure (Distal Ulna Resection) Instability of the ulnar stump may develop resulting in radioulnar impingement. Younger patients may complain of weakness. Ulnar translation of the carpus may occur in rheumatoid patients. Figure 21-1 In the nonrheumatoid patient leave the retinaculum intact distal to the ulnar styloid to help maintain EDQ and extensor carpi ulnaris (ECU) stability.
Indications
Pitfall
Technique
Pearl
Related posts:
 Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
 Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
 Sauve-Kapandji Procedure
Sauve-Kapandji Procedure
 Flexor Carpi Radialis Tendon Stabilization of the Scapholunate Joint (Brunelli Procedure)
Flexor Carpi Radialis Tendon Stabilization of the Scapholunate Joint (Brunelli Procedure)
 Closed Reduction and Internal Fixation of Bennett’s or Rolando’s Fractures
Closed Reduction and Internal Fixation of Bennett’s or Rolando’s Fractures
 Capitate Shortening with Capitohamate Fusion
Capitate Shortening with Capitohamate Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


