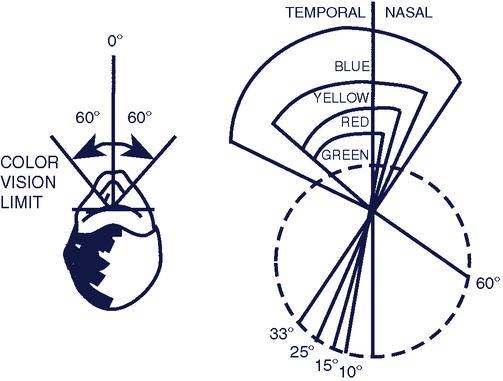
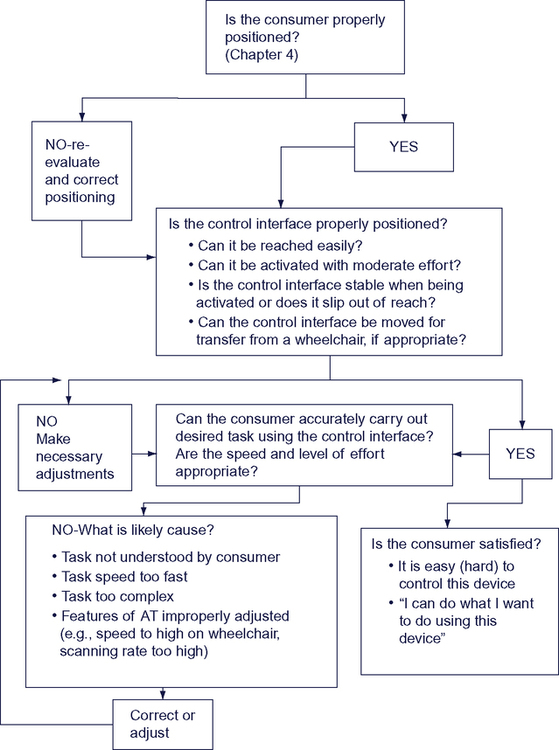
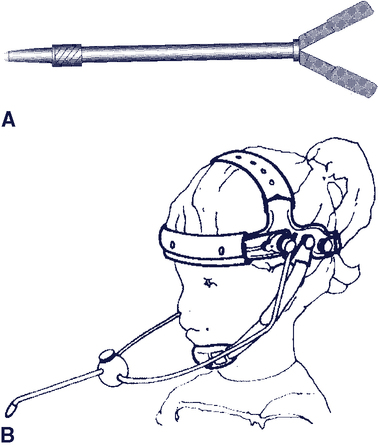
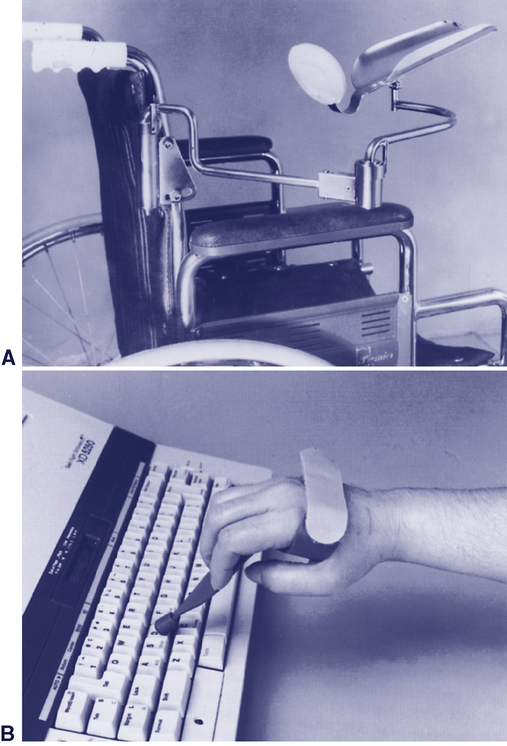
Upon completing this chapter, you will be able to do the following: 1. Describe the elements of the human/technology interface and its role within the assistive technology component of the HAAT model 2. Describe the characteristics of control interfaces 3. Discuss a framework for control interface evaluation 4. Identify technologies for direct selection The user of an assistive device activates a control interface to provide an input to operate the device (e.g., turn it on, make a selection, or make it talk). Control interfaces come in many different sizes and shapes. The user’s needs and activities dictate the type of control interface that is chosen. The user’s needs are those elements of their motor, sensory, and cognitive abilities that influence the successful use of a control interface. User’s activities include a variety of tasks such as turning on a light using an enlarged light switch, or accessing a portable communication system using a single switch. In order for the person to know that they have successfully activated the device, it is necessary for there to be feedback from the device to the person. This usually takes place through a visual or auditory display or both. These displays are considered a component of the human/technology interface. Alternative displays for people with visual or auditory impairments are discussed in Chapters 8 and 9, respectively. Control interfaces differ according to their spatial, sensory, and activation characteristics.4,8 Consideration of these characteristics can be helpful when working to optimize the effectiveness of a particular device for an individual. The important factors are the placement and size of the control interface (which we call spatial characteristics), how the person uses the control interface to make a selection (activation characteristics), and what feedback is obtained as a result of the person using it (sensory characteristics). These characteristics and their use in control interface assessment and recommendation is discussed in detail by Cook and Polgar (2008).8 The target size and spacing should be matched to the individual’s fine and gross motor skills. Targets that are large and spaced far apart are useful for individuals with good range of motion but limited fine motor control (e.g., someone with a coordination disorder or a tremor). Small, closely spaced targets are useful for individuals with limited range of motion, muscle weakness, and accurate fine motor control (e.g., someone with arthritis). For example, a single control interface has one target, and the target size is the dimension (height and width) of the control interface (see Figure 6-10, A, for example). Typically, a single control interface can accommodate an individual who has limitations in range of motion and limited fine motor control. Control interface arrays (including joysticks) have two to five switches, each representing a different target and a different result when activated. The user’s range of motion required to access a switch array needs to be larger than for a single switch, but it can still be relatively small, depending on the spacing between the switches. The user’s fine motor control needs to be more refined than that required for a single control interface and less refined than that for a keyboard. There are many characteristics related to the activation of the control interface.8 The effort expended and the amount of movement required to activate the control interface are important to consider when evaluating how effective a control interface is for an individual or when troubleshooting a situation that is not working well. Deactivation or the release of a control interface may be different than activation and also needs to be considered. While the choice of a control interface for a given individual will be part of the team assessment, the rehabilitation assistant (e.g., OTA, PTA) will often be the one interacting with the user on a regular basis. This frequency will allow the rehabilitation assistant to see if the person is able to use the device easily or if some adjustments are needed. Control interfaces can be activated by a variety of methods that are shown in Table 6-1. The first column identifies the three ways the user can send a signal to the control interface (i.e., movement, respiration, and phonation); the middle column shows how each of these signals is detected by the control interface; and the column on the far right provides examples of each type of control interface. Table 6-1 The second type of body-generated signal shown in Table 6-1 is respiration. The signal detected is either airflow or air pressure. The use of this type of control interface, generally called a sip-and-puff switch, requires that the user be able to place and maintain her lips around a tube and produce good control of airflow. There is also a force required to release, or deactivate, some control interfaces. Muscle contraction is necessary to remove, or release, the body part from the interface. Weiss (1990)17 measured both activation and deactivation forces for several mechanical switches and found that force was required to release the control interface in all cases, but the deactivation force was approximately one third to one half that required for activation. The eye is sensitive to colors in the visual spectrum (from violet to red), but the eye is not equally sensitive to all colors in this range. If the eye is fixed and not allowed to rotate, the limits of color vision are 60 degrees to each side of the midline. Within this range, the response of the retina to colors is not equal for all wavelengths (colors). Figure 6-1 illustrates that blue objects are visible over the entire 60-degree range, whereas yellow, red, and green are recognizable only at points closer to the fixed (center) point of vision. This limitation on color sensitivity has a practical implication when working with individuals who rely on peripheral vision or who have difficulties in moving their eyes to track objects. If a target (e.g., a switch) is green or red, its position may limit the person’s ability to see the object. We can increase the visibility of the switch by using blue or yellow. Somatosensory feedback is the tactile, kinesthetic, or proprioceptive input sensed on activation of the control interface. For example, the texture or “feel” of the activation surface provides tactile data. The position in space of the body part and its movement when the user activates the control interface provides proprioceptive feedback. Many mechanical control interfaces require movement and force for activation. The displacement of the control interface provides kinesthetic (movement) feedback, as well as tactile and proprioceptive feedback that are beneficial to the user. If there is not much movement, as with a membrane keyboard or touch screen, the sensory feedback is less and the individual may press harder than necessary, thinking that more force is needed to activate the keys. This extra, sustained force may result in errors, since many keyboards will repeat entries if a key is pressed for more than a second or two.* Selecting a control interface for an individual is a complex process.8 Once a control interface is selected and implemented for an individual, its effectiveness must be evaluated on an ongoing basis. The evaluation of effectiveness may be at the time of initial use or at any point where a change has occurred. The desired change in control method may be due to the individual (e.g., a degenerative condition that makes use a particular control interface difficult). Alternatively, the change may be required due to a change in technology. For example, a new wheelchair may be acquired and the control interfaces will have to be mounted to the new wheelchair and set up for the user, or the new wheelchair may use a different control interface to operate it. A new device to be controlled (e.g. a more advanced augmentative communication system) may be introduced, requiring changes in the control interface. Finally, the consumer may be experiencing difficulties (poor accuracy, excessive fatigue) using the control interface for the desired activities. In all of these cases, reevaluation of effectiveness is required. Evaluating the effectiveness of a control interface that has been selected and installed can be challenging because of the large number of factors that can be involved. Figure 6-2 shows a systematic approach to evaluation of how well a control interface is working for an individual consumer. The process includes observation of the consumer carrying out the desired tasks. The range of possible tasks for which a control interface might be used includes controlling a power wheelchair (Chapter 12), making choices with an Electronic Aid to Daily Living (EADL; Chapter 14), using an augmentative communication system (Chapter 11) or cognitive assistive technologies (Chapter 10), or providing input to a computer as we discuss later in this chapter. The person and the control interface should both be positioned to maximize function. The importance of proper positioning to maximize an individual’s function is discussed in Chapter 4. A person’s position should be observed as he or she uses a device to be sure that activation of the control interface does not result in an undesirable change in body position. If inadequate positioning appears to be affecting the person’s ability to control an interface, it should be addressed. The position of the control interface can also affect the person’s ability to activate it, and changing the height or the angle of the control interface even slightly may dramatically improve the person’s control ability. For individuals who lack functional movement in their arms and hands, a mouthstick or head pointer (Figure 6-3) can be used with head and neck movement to access a keyboard or perform other types of direct selection tasks (e.g., dialing a telephone number or turning pages in a book). A mechanical head pointer is a rod with a rubber tip that is attached to a head band. The individual can use the end of the head pointer to depress keys. Besides being able to move the head vertically and horizontally, the individual must have the ability to move the head forward to depress keys. Hand pointers (Figure 6-4, B) can be grasped with a gross hand grip. These devices include a projection with a rubber tip that can be used to press keys. These are sometimes referred to as typing aids. A pointing aid may help an individual who has the gross motor ability to move her arm and hand around a keyboard but has difficulty extending and isolating a finger to depress a key. There are commercially available aids that can be strapped onto the hand to assist in pointing, such as the typing aid shown in Figure 6-4, B. In some cases it is necessary to custom fabricate a pointing aid in order for it to fit the consumer’s hand appropriately. These custom-fabricated aids can range from complex hand splints to simple tools, such as a pencil with an enlarged eraser. Mouthsticks are often used by individuals with quadriplegia as a result of a spinal cord injury. A mouthstick consists of a pointer attached to a mouthpiece. The user grips the mouthpiece between his teeth and moves his head to manipulate control interfaces or other objects. The shaft of the mouthstick can be made from a wooden dowel, a piece of plastic, or aluminum. In some cases, interchangeable tips for different functions (e.g., painting, writing, or typing) can be inserted into the distal end of the shaft. The mouthpiece can be a standard U shape that is gripped between the teeth or a custom-made insert. Mouthsticks are also available from several suppliers.* Use of a mouthstick requires good oral-motor control; later in this chapter we discuss training to develop these skills. Individuals who have weakness in the arm may not have enough strength to access the full range of a keyboard adequately. A mobile arm support (Figure 6-4, A), which props the arm and assists in arm movements by eliminating some of the effects of gravity, may then allow the individual to access a keyboard. Several direct selection approaches utilize on-screen keyboards that employ a video image of the keyboard on the video screen, together with a cursor (see Figure 7-1, A). The user makes choices by moving the cursor to the desired key and selecting it (e.g., by clicking). A variety of mouse pointing methods or scanning can be used to position the cursor and make a selection (see Chapter 7). The critical questions presented in Box 6-1 can assist in determining the effectiveness of a keyboard for a specific individual. Affirmative responses to all seven questions indicate that the control interface is meeting the consumer’s needs. A negative answer to any one or more questions will direct the rehabilitation assistant’s attention to the area or areas needing attention. If the answer to any of the questions in Box 6-1 is determined to be “no,” then the use of a less limiting keyboard, a control enhancer, or modifications to the keyboard should be considered. For example, if a standard keyboard cannot be used because of a targeting problem, we may consider the following: (1) an enlarged keyboard with larger targets (less limiting), (2) a keyguard (modification), or (3) a typing aid (a control enhancer). For written communication, a keyboard is typically considered the most efficient means of inputting information. The standard keyboard is the first choice for computer access. However, many individuals with disabilities are unable to use a standard keyboard. Fortunately, there are a number of alternatives. Table 6-2 provides examples of some commercially available alternatives to the standard keyboard. Table 6-2 Alternative Keyboards for Direct Selection Data from: RiverDeep, San Francisco, Calif. (http://rivapprod2.riverdeep.net/ ); Able Net, Inc., Minneapolis, MN, (http://www.ablenetinc.com/); Laureate Learning Systems, Inc., Winooski, Vt. (www.laureatelearning.com); IntelliTools, Frederick, CO (www.intellitools.com); Inclusive Technologies, (http://www.inclusive.co.uk/catalogue/index.html); In Touch Systems, Spring Valley, N.Y. (www.magicwandkeyboard.com); Maltron-USA (http://www.maltron-usa.com/expanded.htm); TASH, Inc., Ajax, Ontario, Canada, or Richmond, Va. (www.tashinc.com). The term repetitive strain injury (RSI) encompasses several musculoskeletal disorders that develop as a result of sustained, repetitive movements.5 Carpal tunnel syndrome is the most common RSI. Standard keyboards place the hands in an unnatural position with the forearms pronated and the wrists extended and ulnarly deviated. This position causes strain on the tendons and nerves. Numerous alternatives to the standard keyboard have been developed in attempts to reduce this strain on the wrist and hands. These alternatives range from minor rearranging of the keys to major redesign of the keyboard shape and configuration. Ergonomic keyboards attempt to reduce the strain placed on the hands and wrists during the repetitive motion of keying by putting the forearms, wrists, and hands in a neutral position, which is more natural and more comfortable for the typist. There are three basic ways in which the standard keyboard has been redesigned. The first and most common type of ergonomic keyboard is the fixed-split keyboard (e.g., Figure 6-5, A). The difference between these keyboards and standard keyboards is that the keys are spaced farther apart and the keyboard is curved, so that the hands are placed in a more neutral position. Many of these keyboards have a built-in wrist rest to support the wrists while typing.
Control Interfaces for Assistive Technologies
Characteristics of control interfaces
Spatial Characteristics
Activation and Deactivation Characteristics
Signal Sent, User Action (What the Body Does)
Signal Detected
Examples
1. Movement (eye, head, tongue, arms, legs)
1a. Mechanical switch: activation by the application of a force
1a. Joystick, keyboard, tread switch
1b. Electromagnetic switch: activation by the receipt of electromagnetic energy such as light or radio waves
1b. Light pointer, light detector, remote radio transmitter
1c. Electrical switch: activation by detection of electrical signals from the surface of the body
1c. EMG, EOG,* capacitive, or contact switch
1d. Proximity switch: activation by a movement close to the detector but without contact
1d. Heat-sensitive switches
2. Respiration (inhalation-expiration)
2. Pneumatic switch: activation by detection of respiratory airflow or pressure
2. Puff and sip
3. Phonation
3. Sound or voice switch: activation by the detection of articulated sounds or speech
3. Sound switch, whistle switch, speech recognition
Sensory Characteristics
Is it working? evaluating the effectiveness of a control interface
Enhancing control: proper positioning and arm supports
Head Pointers, Hand Pointers, and Mouthsticks
Mobile Arm Supports
Control interfaces for direct selection
Keyboards
Category
Description
Device Name/Manufacturer
Expanded keyboards
Generally membrane keyboards that have enlarged target areas, often programmable so that key size can be customized; useful for individuals with good range and poor resolution; also useful for individuals with limited cognitive/language skills or visual impairment.
IntelliKeys (IntelliTools); USB King Keyboard (TASH, Inc.); Expanded Keyboard (Able Net, Inc.); Big Keys Plus (Inclusive Technologies); Expanded Keyboard (Maltron)
Contracted keyboards
Miniature, full-function keyboards, typically with membrane overlay; useful for individuals with limited range of motion and good resolution.
USB Mini Keyboard (TASH, Inc.); Mini Keyboard (Able Net, Inc.); The Magic Wand Keyboard (In Touch Systems)
Touch screens/touch tablets
Activated by either breaking a very thin light beam or by a capacitive array that detects the electrical charge on the finger; the electrode array used to detect where the finger or pointer is touching is transparent; touch screen can be placed over the face of a monitor.
Touch Window (RiverDeep); MagicTouch (Laureate Learning Systems, Inc.)
TongueTouch Keypad
Battery-operated, radio frequency–transmitting device with nine pressure-sensitive keys activated by tongue; universal controller processes information sent from keypad to receiver.
Special-purpose keyboards
Keyboards on special-purpose devices, such as augmentative communication and environmental control devices; available keys may be much more limited in number or may be specific in function compared with standard keyboard.
See Chapter 11
Ergonomic Keyboards

Related posts:
 Delivering Assistive Technology Services to the Consumer
Computer Access – Augmenting the Keyboard and Mouse
Introduction and Overview
Sensory Aids for Persons with Auditory Impairments
Technologies That Aid Manipulation and Control of the Environment
Sensory Aids for Persons with Visual Impairments
Delivering Assistive Technology Services to the Consumer
Computer Access – Augmenting the Keyboard and Mouse
Introduction and Overview
Sensory Aids for Persons with Auditory Impairments
Technologies That Aid Manipulation and Control of the Environment
Sensory Aids for Persons with Visual Impairments
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Control Interfaces for Assistive Technologies