Congenital Coronary Artery Abnormalities
David J. Driscoll
NORMAL CORONARY ANATOMY
The left main coronary artery divides into the left anterior descending (LAD) coronary artery and the circumflex coronary artery (Fig. 281.1). Branches of the LAD coronary artery include the left conus, septal, and diagonal arteries. Branches of the circumflex coronary artery may include the sinus node artery, the Kugel artery, marginal arteries, and the left atrial circumflex artery.
Branches of the right coronary artery (RCA) include the right conal branch, the sinus node artery, an atrial branch, the right ventricular muscle branches (including the acute marginal branch), the posterior descending coronary artery, the atrioventricular node artery, and septal branches (Fig. 281.2).
MAJOR CORONARY ANOMALIES
Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery
Anomalous origin of the left coronary artery (ALCA) from the pulmonary artery may be the most common important coronary anomaly with which pediatricians and pediatric cardiologists must deal. A patient with ALCA may present with signs and symptoms of myocardial infarction and congestive heart failure in infancy or be detected serendipitously in adulthood or at autopsy. Subjects with well-developed collateral connections between the RCA and left coronary artery (LCA) systems may not develop myocardial infarction and may do well, but subjects with poor collateral circulation may have myocardial infarction and present in infancy. In the immediate newborn period, pulmonary artery resistance and pressure are increased, flow through the anomalously arising LCA is antegrade from the pulmonary artery, and myocardial perfusion is adequate. As pulmonary resistance and pressure decrease, antegrade flow of blood from the pulmonary artery through the LCA decreases, and myocardial infarction can occur. Clinical features of ALCA in infancy are similar to those of myocarditis and cardiomyopathy, and the diagnosis of ALCA must be considered in the differential diagnosis of unexplained congestive heart failure in infancy. In teenagers and adults, the presence of ALCA may be suspected in the presence of unexplained cardiomegaly, mitral insufficiency, or continuous cardiac murmur. Angina may occur. The ideal treatment of ALCA is to detect the presence of the anomaly before myocardial infarction occurs and to establish a coronary system that prevents myocardial infarction. However, most cases in infancy come to medical attention only after myocardial ischemia and infarction have occurred. Treatment consists of surgically establishing a two-coronary artery system originating from the aorta. Several techniques to accomplish this system have been described. Infants with evidence of acute myocardial infarction should be treated with oxygen, sedation, rest, digitalis, and diuretics while awaiting definitive operation.
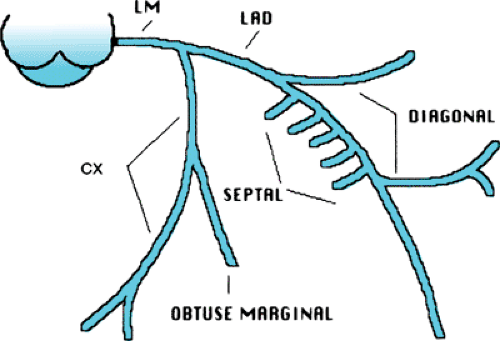 FIGURE 281.1. Normal left coronary artery system. CX, circumflex; LAD, left anterior descending; LM, left main. |
Anomalous Origin of the Left Coronary Artery from the Right Sinus of Valsalva
ALCA from the right sinus of Valsalva or from the proximal RCA is a rare but important malformation because it is
associated with sudden death. Patients in whom the aberrantly arising LCA passes between the aorta and the pulmonary artery appear to be at the greatest risk for sudden death. Usually, patients are asymptomatic until sudden death occurs, although some patients may have symptoms of angina or coronary insufficiency. Symptoms may include syncope or lightheadedness associated with exercise. This diagnosis must be considered in children and adolescents with angina-like chest pain or syncope/presyncope associated with exercise.
associated with sudden death. Patients in whom the aberrantly arising LCA passes between the aorta and the pulmonary artery appear to be at the greatest risk for sudden death. Usually, patients are asymptomatic until sudden death occurs, although some patients may have symptoms of angina or coronary insufficiency. Symptoms may include syncope or lightheadedness associated with exercise. This diagnosis must be considered in children and adolescents with angina-like chest pain or syncope/presyncope associated with exercise.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


