Compensatory and social justice: societal sources of claims for health care
Objectives
New terms and ideas you will encounter in this chapter
compensatory justice
stigma
workman’s compensation
collective responsibility
communitarian approach
interdependence
altruism
reciprocity ethic
social need
labeling
“the dilemma of difference”
vulnerability
social marginalization
solidarity
personal responsibility for health
Topics in this chapter introduced in earlier chapters
| Topic | Introduced in chapter |
| Beneficence | 4 |
| Nonmaleficence | 4 |
| Distributive justice | 15 |
| Social justice | 15 |
| Equity | 15 |
Introduction
Justice issues often are difficult to grasp because they require professionals to move beyond their usual one-on-one interaction to consider the well-being of whole groups of people. As you learned in the previous chapter, distributive justice focuses on medical conditions as the basic approach to justly allocating resources. This chapter introduces two other related dimensions of justice that are pertinent in some of the situations you will face as a health professional. Compensatory justice and social justice (introduced in Chapter 15) both arise from the observation that not everyone has the same chance as others to benefit from basic societal services and goods. The similarity between the two types of justice is that each takes into account additional factors to medical conditions, those factors being related to the person’s or group’s relatively disadvantaged position in society. Compensatory justice has built into it an assumption that the person or group at least has a role (e.g., worker) that is valued by mainstream society. In contrast, social justice is a “no fault” position that says regardless of social role it is simply the societal disadvantage that matters. The assumption is that a well-working society has to respect everyone where they are and try to make adjustments regarding who needs what. At the core of the issue for our study here is the concern that some groups of people have health problems related to their disadvantaged position in the larger society. We devote most of the study in this chapter to compensatory justice but also demonstrate how it is one aspect of the broader concept of social justice, the latter of which focuses on serious disparities in health and health care allocations.
The story of the Maki brothers is an example designed to help you focus on how social contexts factor into compensatory justice considerations and how you, the health professional, are involved.
The Story of the Maki Brothers

Mr. Eino Maki is an asbestos miner who emigrated from Finland to the United States in 1975. He was born into a poor rural family that lived in a small remote village near the Russian border. Eino did not attend school in Finland after the first grade because he was a “slow learner” and could not keep up with the other students. Although most students in his country received excellent educations, his family refused to send him to a special school in Tampere, some 300 miles away, saying they needed his help on the farm.
One dreadful morning in 1972, a fire destroyed the family’s home and Eino’s parents perished in the fire. Eino and his sister were sent to live with an aunt and uncle in Helsinki. At the age of 18 years, he could not find work in Helsinki, so he emigrated to the United States to live with his unmarried older brother in an area where there are many asbestos mines. The community where his brother lives is about 90% Finnish.
When Eino arrived in the United States, his brother John attempted unsuccessfully to find him a job in the railroad construction company where he was employed as a section worker. After several months, Eino did secure a job in a nearby asbestos mine.
He has been employed by this same mining company and has held essentially the same position for the last 36 years. Although at work he still suffers the ridicule at times associated with his being “slow” at grasping ideas, he is an excellent worker and participates in the social life of the community. Many evenings at the local bar, the men spend time reminiscing about the “good old days” in Finland, and everyone talks about going back. Privately, however, John and Eino agree that it is unlikely they will ever return.
In the last 2 or 3 months, Eino has had increasing difficulty breathing. Occasionally, he has coughed up blood-tinged sputum, and he often has pains in his chest when he awakens, but they disappear after he has been up and around for a couple of hours. At first, he does not say anything to John, but one November morning he realizes that he cannot make it to work. He asks John to take him to the company physician.
Eino has never liked doctors. In all of his years of employment, he has visited the company clinic only for the required routine annual physical examinations and once when he suffered a dislocated shoulder in a fall from a mine platform. He has always passed the physical examinations with a “clean bill of health.”
After the examination, the physician assistant who conducted the initial tests tells Eino that some further tests are needed and for them he will have to be admitted to a hospital, which is about 120 miles away. Eino is angered at this news but realizes that he cannot go back to work feeling the way he does. He tells John he wants to rest at home until he feels better, but John, seeing the trouble his brother is having, insists he goes and drives him there.
Five days later in the hospital, Eino takes a sudden turn for the worse. John is called and drives back to the hospital. When he arrives, he is met by Dr. Kai Nielson, a young physician who looks to John as if he cannot be a day older than 16 years. Dr. Nielson invites John into a little room next to the nurse’s desk and closes the door. “Mr. Maki, I’m afraid I have some bad news,” he says. “Your brother has not been told yet, but he has cancer and has had it for quite a long time. Ideally, we should start a type of treatment immediately that his company’s health plan does not totally cover.”
So far, John has barely been hearing what the young doctor is saying. His mind is racing wildly. He vaguely recalls Eino’s report of a discussion at a union meeting a year or so ago regarding a rumor that work in the asbestos mines causes cancer and that their union was looking into it. This concerned John greatly, but Eino brushed it aside and said it was “a bunch of hogwash” and he was “healthy as a horse,” refusing to discuss it further. Later he told a friend, “you know that Eino is not only healthy as a horse but stubborn as a mule. What could I do? I let the matter drop.”
Finally, John realizes that Dr. Nielson has been talking to him. “We could do the treatment, but unless Eino has additional insurance coverage, the treatment is going to cost him a lot of money.”
John tells the physician that they own a small cottage together, with about two acres of unfarmed land around it. They have no savings, only the pension that their respective companies provide, but that benefit cannot be realized until Eino is 65 years old. Dr. Nielson replies sympathetically, “Well, there is a chance your brother will be eligible for federal assistance, but unfortunately it may mean you will have to sell your house to become eligible for it once you’ve expended the earnings you’d realize from that. I don’t know exactly how it works, but I’ll have the social worker talk to you. Of course, we can’t guarantee that the treatment will beat the disease, but we feel reasonably sure that it would at least slow down the rate of growth of the cells.”
There is a pause. Then he adds, “It is, of course, a big decision. It is entirely up to you and your brother what you decide to do. We haven’t talked to him or, rather, been able to talk to him. He doesn’t like doctors much. Why don’t you two talk it over with the social worker here or the physician assistant he saw back at his company clinic? Remember, it’s your decision and your brother’s. But don’t take too long in deciding. . . .I think every day counts. Do you have any questions?” John shakes his head “no.” “Well,” Dr. Nielson concludes, “if you do after talking with the others I’ve recommended, have them set up an appointment for you to see me again.”
As John stands, Dr. Nielson extends his hand and John shakes it warmly. John glances up into the doctor’s face and sees genuine compassion in the young man’s eyes. John blurts out, “Was the cancer caused by the mines?” The young doctor drops John’s hand and studies his own hands as he answers, “Mr. Maki, the cause of cancer is often complex. It can be the result of a combination of factors. But the type of cancer that your brother has is the same type that asbestos miners get at a higher rate than the general population. Primarily it attacks the lungs.”
John thanks Dr. Nielson. Outside the doctor’s office, he wanders over to a window and stares outside into the snowy darkness for a long time, his hands in the pockets of his overalls. He has not cried since their brother Matt was killed in a tractor accident many years before, but he feels a lump rising in his throat now. He feels totally unable to move, as if he is glued to the floor. He struggles to think clearly, but his mind remains a blank.
The story of jane tyler and sam puryo

Jane Tyler, a 32-year-old single woman and mother of three children (5, 8, and 12 years old), has been living on public assistance since her first child was born. Jane lives in a small apartment above her mother’s in a part of town most people never go. Her mother helps with light housekeeping and child care. Now that all three children will be in school, Jane has successfully applied for a grant from the local Woman’s Fund, a private organization, that will allow her to train to become a business information technology assistant so that she can make a living for herself and her family. Receiving this award was a tremendous boost to her self-esteem, and she sees it as a bright doorway out of her “no exit” life situation. The one nagging anxiety she is experiencing is a severe shortness of breath at times and unusual fatigue. Before taking on this additional load of schooling, she decides to have a checkup at her neighborhood clinic.
It comes as a devastating blow to her to learn that she has emphysema. She has been threatening to stop smoking for a long time, but her two pack-a-day habit has had a strong grip on her. It is an even greater shock to learn that although the emphysema is only in the beginning stages, she may not be eligible for state-of-the-art curative treatment because she is on public assistance. The state legislature presented to the voting public the opportunity to decide priorities for high-cost interventions provided through public funds by sending a questionnaire to a sample group. (Some readers will recognize this general approach as the innovative tactic passed by the Oregon state government in 1989 that became known as “The Oregon Experiment.”) Three physicians concur that Jane’s smoking is a direct cause of her emphysema. One of them believes there may be cofactors that lead some people to actually manifest the symptoms of emphysema, whereas others do not. The other two are completely convinced her smoking directly has created her serious health problem. Because two of the physicians of the three are needed for this policy to take effect, she is able to receive only cursory treatment. Her only opportunity for an adequate treatment regimen is for her to find some way to pay for it.
Sam Puryo is a caseworker in the public assistance office. Jane has been one of his clients for several years. He is upset at what he judges to be the apparent injustice of the laws that have put her in her current dilemma. He tries to call his state senator to see whether there are any loopholes in the law that could help her or whether an exception can be made for this woman who Sam sees as exceptional. The senator is not encouraging; she is sympathetic but knows of no loopholes and is pessimistic about an exception being made.
During a coffee break, Sam gets into a discussion of the new rulings with his colleagues at the welfare office. His fellow social worker is strongly in favor of the approach taken by the legislature. All the people at lunch agree that it is important to be willing to consider the arguments.
The story of John and Eino Maki raises numerous ethical questions. For instance, some people reading this story have questions about confidentiality. Why is Kai Nielson sharing all of this potent information with John when Eino, a competent adult, is the patient? What about Eino’s informed consent? Is it appropriate for the physician to put the burden of sharing the bad news with Eino on John’s shoulders? What should the role of the physician assistant and social worker be? These are certainly important ethical questions. However, we beam our lens in this chapter on the justice issues that patients in similar situations to Eino’s raise. Their basic similarity is that they are among the members of society who are dismissed or even disdained by members of mainstream society even though they contribute in ways that society needs for its overall well-being.1
The goal: a caring response
Eino Maki, a seemingly healthy, hard-working man, becomes a victim of circumstances that leave his health compromised. A caring response by health professionals requires that they do whatever is “best” or, in the language of ethics, is beneficent for this patient. In the story, the physician assistant and Kai Nielson have been doing exactly that in their attempt to get at the clinical root of Eino’s symptoms, and they each make strong recommendations about what he needs to do. At the same time, they know that matters are fast slipping out of their hands. There is an environmental source of his cancer, a death-dealing cancer we presume, triggered by his employment in a company where he likely has been exposed to toxic levels of asbestos over a prolonged period of time. Mr. Maki’s decision about what to do for his cancer treatment will depend in part on the availability of funds from his employing company or a government source to help pay for them. If the professionals think this through to its logical conclusion, they will realize that a caring response requires that they try to help build and strengthen institutions and societal arrangements that support individuals in such predicaments. Involvement at this level is aimed at policies that reflect justice for groups of people who are societally disadvantaged. The “Eino Makis” do not have the same opportunity to choose among desirable job options to the extent that persons who are better situated financially and socially do. Such policies are not designed only for one person (e.g., Mr. Maki) the way a treatment plan is created for a specific patient but outline a program that covers him and others like him. There is a subgroup of institutional and social arrangements that address legal mechanisms to compensate persons for harms incurred in the larger environment whether workplace, home, or publicly shared spaces. Compensatory justice deals with this reality from an ethical and legal standpoint, and it is the ethical considerations we consider here.
The six-step process in compensatory justice decisions
In Chapter 15, you studied about allocation dilemmas when whole groups of individuals become eligible for goods or services because of their medical need.
Now the lens of justice turns to include an additional question. What ethical difference does it make when a patient’s medical need is caused by injury or illness but this person’s condition is also caused by his societal position and the lifestyle people in that position have? Eino Maki is one excellent example. He is carrying out a type of work that is dangerous to his health but remains in a job available to him and others who have similar low social and economic status in society. You might respond that others who are at more financially secure levels of society have an opportunity for this kind of work too. True, but this reasoning is akin to the French political philosopher during the French Revolution who observed that “both the rich and the poor have an equal right to sleep under the bridges of Paris at night.” Eino’s autonomy to select a safer or more pleasant work environment is greatly diminished or absent.
Thoughtful individuals have pondered the role that such societally determined differences among patients should play. To help elucidate some of their thinking, let us first consider the relevant information in the story of the Maki brothers.
Step 1: gather relevant information
We are making an assumption that Eino’s situation is caused by his work environment. We can do that for the purpose of encouraging you to think about compensatory justice situations, but of course, in an actual clinical evaluation, your gathering of relevant information first requires clarifying further his stage of lung cancer and whether tests substantiate the source being the asbestos to which he has been exposed as a mining company employee.
Another relevant piece of information that is a question we would have to explore is how much responsibility the company took to help prevent undue exposure. The way risks were presented and action taken to minimize them could make a difference in how we view this situation.
We do know that Eino, and people like him, carry out labor tasks and other societal functions that are needed for the society to function well but often are not valued in other ways and may carry high risks to the workers. Of course, some “high-risk” situations are respected, and individuals who carry out the tasks are given extra financial benefits, and a high status. Examples are firefighters, members of a police force, or U.S. Navy Seals. Others, like Eino, are relegated to greater risk and “less desirable” jobs because of their overall lower social status, often accompanied by poverty or other characteristics that carry a stigma with them. Stigma in this social sense is a term first used by Goffman,2 a sociologist, to depict persons held in low regard because of qualities they have. Status comes into being when mainstream society members, those in control and authority, make arbitrary judgments about the value of different kinds of lives and assign low priority to some whom they devalue. The most explicit negative effect on stigmatized groups comes through their disproportionately small allotment of the society’s goods and services. It can be argued that even if Eino did have the full cognitive capacity to comprehend the danger he was in, he would have been able to do little to change his situation.
Step 2: identify the type of ethical problem
The idea of “compensation” at the root of compensatory justice issues arises out of society’s consciousness that it is the morally right thing to be fair. But not everyone has the same chance at basic lifesaving or life-enhancing benefits from the get-go. Some people are born into situations that, through no fault of their own, force them into a disadvantageous societal position. You are probably familiar with the idea of a “handicap” among competitors in the sports arena. In that environment, good sportsmanship dictates that the handicapped player be given additional “points” to try to make up for the disadvantage. There is an intuitive correctness about this attempt to “even the playing field.” But this compensation activity is not always the case in the larger society, so it is not surprising that the problem it raises is characterized as a dilemma of justice.
Compensatory justice acknowledges due regard for groups of individuals by offering them compensations for harms occasioned by their basic societal disadvantage. The compensation is not necessarily to make up for a consciously perpetrated wrong by another person or society, though one application is criminal justice situations where the perpetrator is required to pay for his or her injury to another. But more generally conceived, it is enough to make it a morally relevant issue that a person or group is vulnerable from the standpoint of having limited access to that society’s available valued goods and services. As for Eino, we have reason to believe that his work in the mines led to a life-threatening, industry-related condition. If the company knowingly placed workers in harm’s way to benefit the company’s bottom line, moral responsibility to redress this wrong squarely can be placed on management. If they, too, are surprised by this bad news, society’s understanding of the wisdom of compensating individuals in such a situation has led to certain mechanisms for spreading the cost of the compensation across the larger society with taxes and other common resources. (In the United States, “workman’s compensation” grew out of this idea originally, but since has come to be considered a protection for anyone injured on a job, no matter their social status, economic security, or other variables.) Sometimes the wisdom of providing compensation has come from pressure by interest groups such as unions or other organizations (e.g., nonprofits run by various religious groups) who try to provide a voice for those who are not in a position to speak effectively against such wrongs themselves. Recently, concern has been expressed in the press and literature that labor unions’ effective voice may be suffering from divided loyalties within the unions themselves.3
However voiced, the idea that a moral claim for compensation should influence how resources are allocated makes this problem a justice dilemma.
Similar reasoning has been applied to priority setting for shelter, food, or other basic goods of society, the underlying assumption being that not everyone comes equally supported by society to adequately take part in life’s basic benefits.
Summary

Compensatory justice assumes that the allocation of resources should be made to address health care problems of an individual or group on the basis of more than medical need alone. Their position in society also is a relevant factor.
Step 3: use ethics theories or approaches to analyze the problem
In Chapter 15, you were introduced to several ethical theories and principles for analyzing the morally appropriate allocation of resources according to distributive justice reasoning. We present two key ones that clearly also apply to the analysis of compensatory justice reasoning: equity and the principle of nonmaleficence.
Equity
To review, equity means that every effort must be made to treat each person in a similarly situated circumstance alike, allowing for departures from that baseline of equality on the condition that differences are derived from ethically acceptable criteria.
For example, Mr. Maki works in a dangerous environment that is not highly regarded as a career line for mainstream members of society. Other miners are “similarly situated.” They are in a class all their own, equal with each other but not with mainstream society. A compensatory justice approach takes into account that mainstream society has more opportunities and resources to deal with crises such as Eino faces. So “similarly situated” means that all like him fall within the same general category of claimants on health care resources. The compensation in the idea of compensatory justice is that there is a moral pull on a just society to respond to the disadvantages that Eino faces as one who is lower on the rung of the social and economic ladder of society through no fault of his own. It may take priority standing or more societal resources to be sure he receives quality care equal to his mainstream counterparts with similar clinical need. The fact that he is contributing an important service that others usually do not choose adds to the argument that those with more resources have a moral responsibility to help the larger society stay intact through compensations to those like Eino who are less well off.
Where does health care as a right fit into the compensatory justice framework? It certainly helps support the idea of compensatory justice if health care is viewed as a right that everyone should have access to in contrast to the opposite idea that health care is a commodity like all other products to be bought by those who can afford to do so. In some cases, the right may require that those who are better off as members of mainstream society are required to do whatever is needed to support access for all.
The principle of nonmaleficence
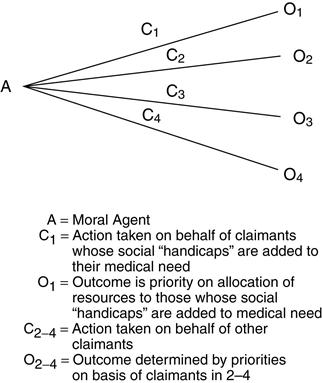
In Mr. Maki’s case, a compelling argument in favor of supporting his medical treatments financially is not only that he has a terrible medical condition (which, indeed, he has) but that he has the condition because he is in a job that carries with it the albatross of a carcinogenic agent that is well established scientifically and can be tested for before damage to a person’s health. Many people examining Eino Maki’s plight have an intuitively sympathetic response in favor of compensating him for his job-related cancer. It seems wrong, from a moral point of view, that he should have to suffer the ravages of a debilitating, painful, and incurable disease because he has been working in a setting that economically disadvantaged individuals are more apt to accept because it is one of the only options open to them and that carries a life-threatening hazard with it (Figure 16-1).
Related posts:
 Surviving student life ethically
Surviving student life ethically
 Ethics theories and approaches: conceptual tools for ethical decision making
Ethics theories and approaches: conceptual tools for ethical decision making
 Morality and ethics: what are they and why do they matter?
Morality and ethics: what are they and why do they matter?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


