I. EMERGENCY SPLINTING OF THE SPINE
A. Patients with spinal injuries should be splinted with a backboard before they are moved, as shown in Fig. 7-1. Immobilize patients with suspected cervical spine injuries by placing sandbags, rolled towels, or rolled blankets on each side of the head. Then put a cravat through or around the backboard (or 3” tape) and over the forehead. In this way, the patient’s head, neck, and backboard can be moved as one unit. Commercial foam as well as plastic neck collars are available in different sizes and are carried by emergency medical technician (EMT) units. One can also make an adequate neck collar by placing foam or felt of the appropriate width, thickness, and length inside a tubular stockinet and then fastening the stockinet about the patient’s neck. This method is particularly useful for immobilizing the neck of injured children where correct sizing is critical so as to immobilize the neck without extension or flexion. The only emergency indication for moving the neck of an individual with a suspected injured cervical spine is to improve an inadequate airway by aligning the neck with the torso and opening the airway with a jaw lift.
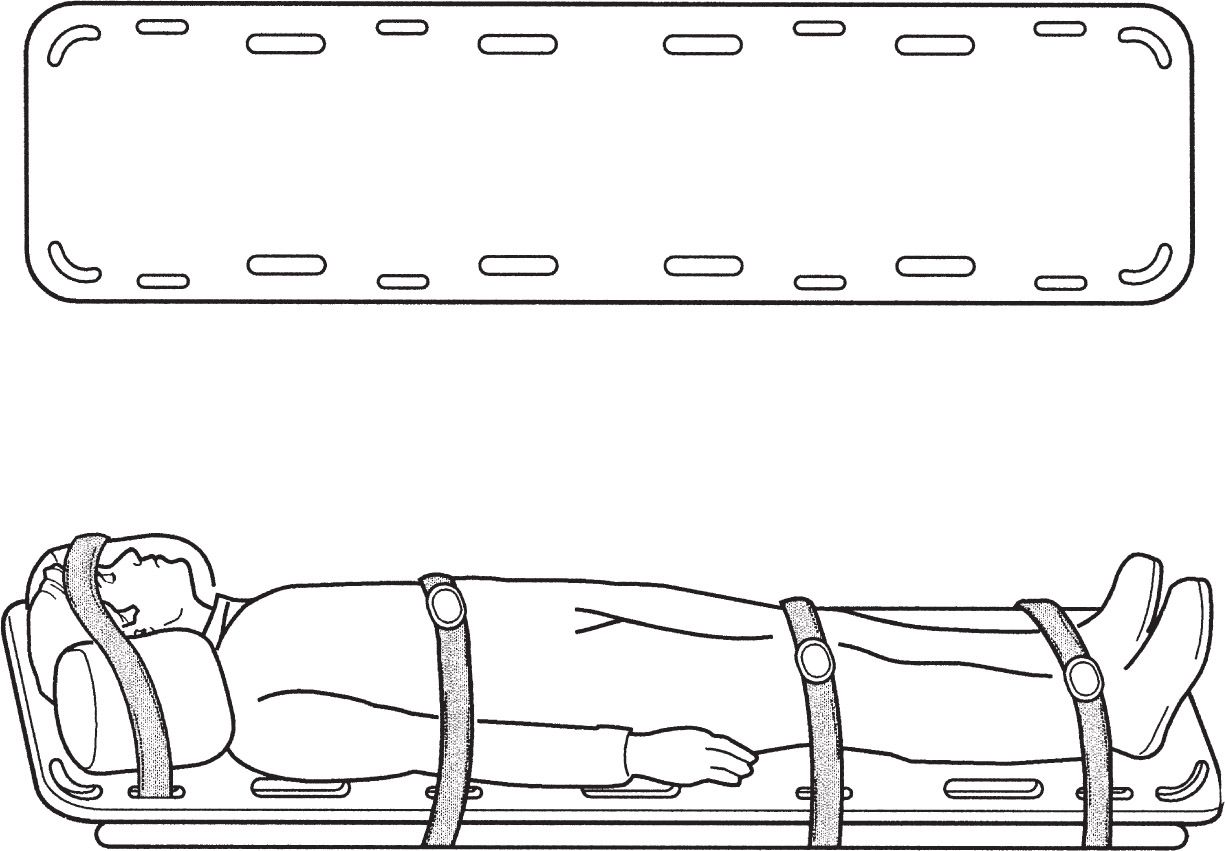
Figure 7-1. A backboard may be used in an emergency to transport a patient with a spinal injury.
B. Be aware of possible neurogenic shock, which is treated by elevating the lower end of the backboard to improve venous return in the reverse Trendelenburg position.
C. If complete evaluation identifies a cervical spine fracture, the patient is usually placed in traction or hard collar immobilization. The direction of traction depends on the injury. If there is no dislocation, a neutral or slightly extended position is preferred (see Chapter 10).
II. UPPER EXTREMITY SPLINTING
A. Remember to remove rings from an involved hand! Swelling can make them impossible to remove without cutting them off and they obscure X-rays. Petroleum jelly can be useful for ring removal.
B. Figure-of-8 splint
- The principal use is for clavicular fractures (see Chapter 14).
- Application. The factory-made figure-of-8 clavicular strap is recommended because it is a webbed fabric and does not stretch. If a properly fitting factory-made strap is not available for children younger than 10 years, make a figure-of-8 strap with a tubular stockinet filled with felt or cotton padding, as shown in Fig. 7-2. These should be used only if they make the patient more comfortable. A sling is generally more effective in this regard. Generally, the figure-of-8 splint does not improve fracture reduction.
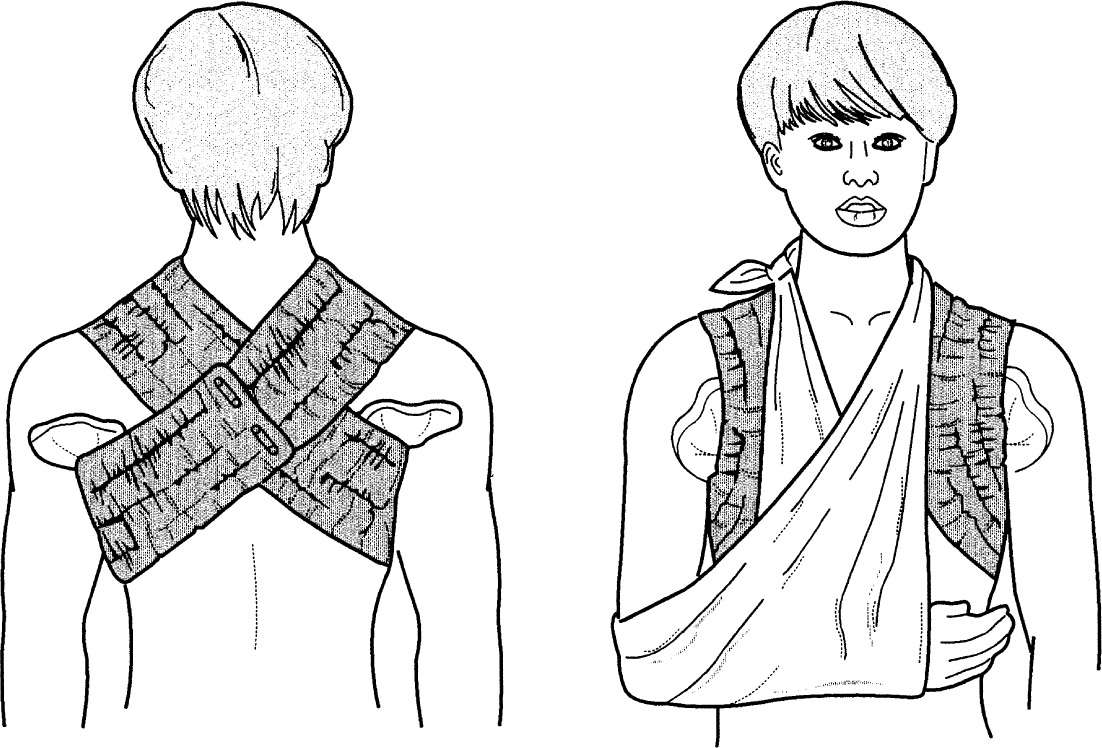
Figure 7-2. Typical figure-of-8 splint made for a child younger than 10 years with a fractured clavicle. In adults, use a factory-made splint when possible.
3. Precautions
a. Prevent skin maceration with a powdered pad in the axilla.
b. In the adult, restrict the use of the sling and encourage glenohumeral motion after 2 weeks to prevent shoulder stiffness.
c. Do not tighten the figure-of-8 strap to the point that the axillary artery or brachial plexus is compressed as manifested by arm swelling and paresthesias.
C. Velpeau and sling-and-swathe bandages
- These bandages are used for shoulder dislocations, proximal humerus fractures, and humeral fractures.
- One application
Related posts:

Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


