Chapter Seven Common sporting illnesses and injuries
Demonstrate care and management of athletes suffering from sporting-related injuries and illnesses.
1. Define and apply the RICER and NO HARM principles.
2. Recognise and manage athletes with hard and soft tissue injuries.
3. Recognise and manage head and spinal injuries.
4. Recognise and manage trunk injuries.
5. Recognise and manage upper limb injuries.
6. Recognise and manage lower limb injuries.
7. Recognise and manage heat and cold injuries and illness.
8. Recognise and manage signs and symptoms of shock.
9. Recognise and manage serious bleeding.
Shock




















Management of shock
 If any signs or symptoms of shock are present, seek medical help urgently.
If any signs or symptoms of shock are present, seek medical help urgently.
 If the athlete is apparently unresponsive, commence the DRSABCD principles.
If the athlete is apparently unresponsive, commence the DRSABCD principles.


 Loosen any tight clothing or protective equipment.
Loosen any tight clothing or protective equipment.
 Protect the athlete from extremes of temperature.
Protect the athlete from extremes of temperature.
 Moisten the athlete’s lips, but do not give drinks or food.
Moisten the athlete’s lips, but do not give drinks or food.
 Continue to monitor the athlete closely as they may deteriorate rapidly.
Continue to monitor the athlete closely as they may deteriorate rapidly.
Serious bleeding
The standard procedure for treating an athlete with serious life-threatening bleeding is:









Hard tissue injuries
Fractures
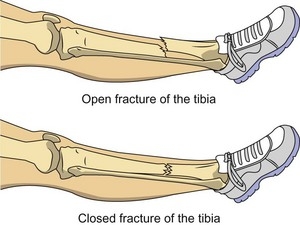
A fracture is an injury where bone tissue loses its normal structure, usually as a result of direct or indirect trauma. There are many different types of fractures; they can be classified according to the type of damage to the bone (e.g.complete/incomplete, displaced/undisplaced) as well as whether the fractured bone penetrates the skin and causes an open wound (open fracture/closed fracture – see Figure 7.1). Fractures can also be classified according to the cause, such as stress fractures, which commonly occur in sport because of overuse or biomechanical problems the athlete might have.
Fractures usually present with:
 the occurrence of a forceful episode
the occurrence of a forceful episode

 being hit by an object or opponent
being hit by an object or opponent
 possible deformity or swelling
possible deformity or swelling












Management of fractures
 Follow DRSABCD principles as appropriate.
Follow DRSABCD principles as appropriate.
 If the athlete is conscious, reassure them and advise them not to move.
If the athlete is conscious, reassure them and advise them not to move.
 Call for an ambulance or medical assistance.
Call for an ambulance or medical assistance.
 Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection.
Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection.
 Check that circulation is present distal to the fracture. If not, call for urgent medical aid.
Check that circulation is present distal to the fracture. If not, call for urgent medical aid.
 If the athlete needs to be moved, immobilise the area of the suspected fracture first.
If the athlete needs to be moved, immobilise the area of the suspected fracture first.
 Immobilise the injured limb in the position you found it.
Immobilise the injured limb in the position you found it.
 Be sure to immobilise the area above and below the fracture.
Be sure to immobilise the area above and below the fracture.

 Check the athlete for other injuries and treat appropriately.
Check the athlete for other injuries and treat appropriately.



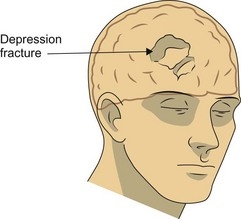
Management of skull fractures
Skull fractures may be characterised by:




Management of skull fractures includes the following steps:
 Rest and prevent the athlete from sustaining possible further harm.
Rest and prevent the athlete from sustaining possible further harm.

 Place the athlete in a position of comfort if possible.
Place the athlete in a position of comfort if possible.

Management of upper and lower arm fractures
 Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection. Apply padding around any protruding bones.
Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection. Apply padding around any protruding bones.



 Check that circulation is present beyond the fracture. If not, call for urgent medical aid.
Check that circulation is present beyond the fracture. If not, call for urgent medical aid.
 Check the athlete for other injuries and treat appropriately.
Check the athlete for other injuries and treat appropriately.


Management of upper and lower leg fractures
 Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection. Apply padding around protruding bones.
Control bleeding if there is an open wound and cover it with a sterile dressing to reduce infection. Apply padding around protruding bones.

 If the ground is supporting the limb adequately there may be no need to splint it to the other limb.
If the ground is supporting the limb adequately there may be no need to splint it to the other limb.
 Check that circulation is present beyond the fracture. If not, call for urgent medical aid.
Check that circulation is present beyond the fracture. If not, call for urgent medical aid.
 Check the athlete for other injuries and treat appropriately.
Check the athlete for other injuries and treat appropriately.

Management of hip fractures





Management of pelvic fractures





Management of rib fractures
 Ensure the athlete is in a comfortable position. If possible, allow them to find their own position of comfort. A half-sitting position resting the affected side on a pillow or cushion is ideal.
Ensure the athlete is in a comfortable position. If possible, allow them to find their own position of comfort. A half-sitting position resting the affected side on a pillow or cushion is ideal.
 Encourage shallow breathing to reduce pain.
Encourage shallow breathing to reduce pain.
 Apply padding over the affected ribs.
Apply padding over the affected ribs.
 Place the arm that is on the same side as the injury over the pad.
Place the arm that is on the same side as the injury over the pad.

 Immobilise the arm using an appropriate sling.
Immobilise the arm using an appropriate sling.

 Be aware that breathing difficulties may be associated with rib fractures.
Be aware that breathing difficulties may be associated with rib fractures.

Dislocations




Management of a dislocation
 Do not attempt to reposition the dislocated joint.
Do not attempt to reposition the dislocated joint.

 Immobilise the injured limb in the position you found it.
Immobilise the injured limb in the position you found it.
 Gently apply a splint and sling. Be sure to immobilise the area above and below the injured joint.
Gently apply a splint and sling. Be sure to immobilise the area above and below the injured joint.
 Check for signs of circulation below the dislocation.
Check for signs of circulation below the dislocation.



Rules for managing dislocations




Soft tissue injuries
 Muscle – muscles consist of cells with a specific function, namely to contract to produce movement of the body. They are usually attached to bones by tendons. Muscles have an extensive blood supply and consequently may bleed heavily when injured. The common injuries that occur to muscle tissue are strains and contusions/bruises.
Muscle – muscles consist of cells with a specific function, namely to contract to produce movement of the body. They are usually attached to bones by tendons. Muscles have an extensive blood supply and consequently may bleed heavily when injured. The common injuries that occur to muscle tissue are strains and contusions/bruises.



 Skin and fatty tissue – an injury to any of these tissues is classified as a soft tissue injury.
Skin and fatty tissue – an injury to any of these tissues is classified as a soft tissue injury.











Process of injury and repair in soft tissue injuries
There are eight stages in the process of injury and repair:
Secondary tissue damage
Additional or secondary tissue damage may be caused by:

















