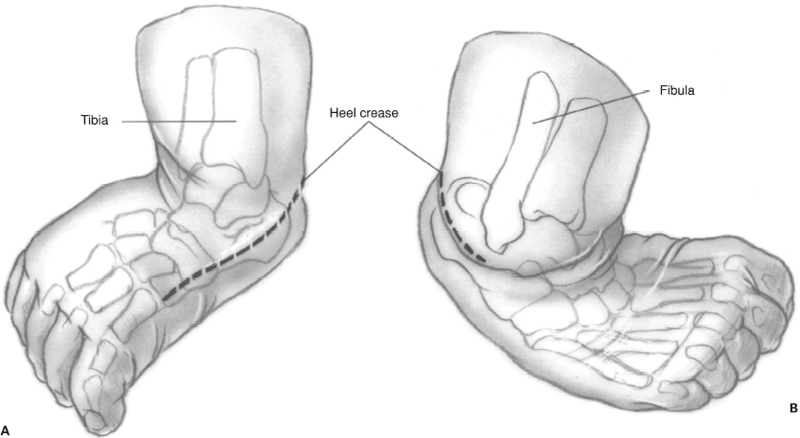
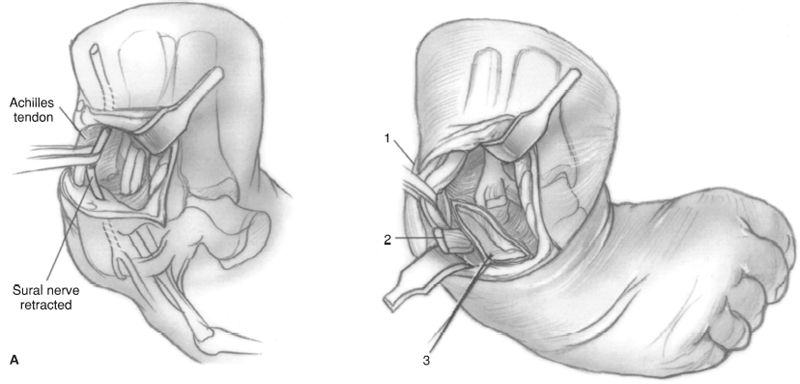
CHAPTER 47 Michael Kuczmanski and John F. Sarwark 1. Rigid clubfoot 2. Foot unresponsive/partially responsive to casting correction 1. If the patient is older than 6 years, correction usually requires bony procedures in addition to soft tissue releases. 2. Revision surgery in severe rigid syndromic clubfeet; in these cases talectomy may be a better option. 1. Attempt manipulation and corrective casting during the first 6 to 8 weeks of life. First correct adductus, then hindfoot varus, and then equinus. 2. Casting allows soft tissue stretching prior to reconstruction even if casting fails. 3. X-rays: weight-bearing anteroposterior (AP) and forced dorsiflexion lateral to assess AP talocalcaneal angle, AP talo-first metatarsal angle, and lateral talocalcaneal angle. 4. Incision options: Cincinnati circumferential incision or Carroll technique with curvilinear medial and longitudinal posterolateral incisions. Both procedures allow access to medial, lateral, and posterior aspects of the foot. The Cincinnati incision is described in the text. 5. The goal of the procedure is to achieve a pain-free, plantigrade foot with near-normal range of motion and function. 1. Place the patient prone 2. Tenotomy scissors 3. Vessel loops 4. K-wires 5. Plain radiography 6. Loop magnification 7. Limb tourniquet 1. Use vessel loops to isolate and protect the neurovascular bundle medially and sural nerve laterally. 2. The degree of deformity dictates the extent of releases necessary (i.e., perform tendoachilles lengthening and posterior capsule release for isolated equinus deformity). 3. Consider releasing the tourniquet if the neurovascular bundle is difficult to identify. Figure 47–1 (A) Skin incision–medial view. Make a transverse incision. This should start at the base of first metatarsal medially. Stay in the dorsal skin, 0.5 cm proximal to the heel crease. (B) Skin incision–lateral view. The transverse incision should extend to the base of the fibula laterally. Stay in the dorsal skin, 0.5 cm proximal to the heel crease. Figure 47–2 (A)
Clubfoot Surgery
Posteromedial and Posterolateral Releases
Indications
Contraindications
Preoperative Preparation
Special Instruments, Position, and Anesthesia
Tips and Pearls
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


