The reconstruction of large bone defects remains a clinically challenging condition. Although many treatment approaches exist, they all have limitations. Recently, bioresorbable polylactide membranes have become commercially available. These membranes, when applied to bone defects, enhance bone healing by direct osteoconduction, exclusion of nonosseous tissues, and enhancing the osteogenic environment for autologous grafts. When combined with appropriate internal fixation and autologous bone graft, bioresorbable polylactide membranes allow for single-step reconstruction of large bone defects.
Large segmental defects remain a challenging clinical problem. Bone defects have many relevant clinical etiologies, such as high energy trauma, periprosthetic osteolysis, tumor resection, or osteomyelitis debridement. The goal of segmental bone defect reconstruction is to restore functional skeletal continuity and maintain soft-tissue function in a timely, well tolerated, and cost-effective manner. No single current technique is reliably successful in the reconstruction of large bone defects. Current strategies for the management of segmental bone defects include autogenous bone grafting, vascularized bone transfer, segmental allograft, demineralized bone matrix grafting, recombinant bone morphogenetic protein grafting, and numerous variants of distraction osteogenesis and bone transport.
Enhancing the local biologic environment to promote bone regeneration has long been recognized as efficacious. In the 1950s and 1960s investigations evaluated the use of nondegradable membranes to promote the healing of cortical defects. The bone growth qualities of bulk porous materials, such as Teflon (polytetrafluoroethylene) and polyurethane sponges, was also studied during this time period. The concept of membranes to enhance spontaneous bone regeneration emerged in the 1970s and 1980s in periodontal and craniomaxillofacial research. Periodontal bone loss has been clinically managed by the use of membranes to allow for the spontaneous regeneration of the periodontal ligament and tooth socket bone in a process that is described as guided tissue regeneration. In addition, there were research efforts at promoting tissue regeneration, such as neural stints and vascular prostheses.
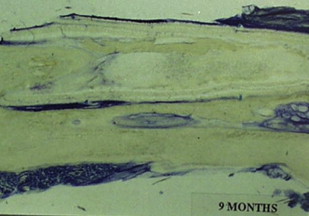
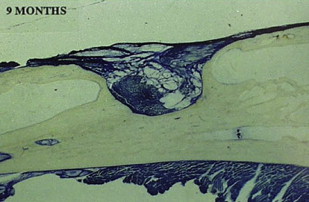
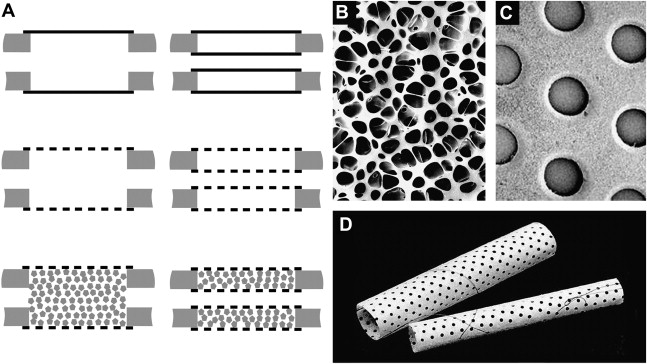
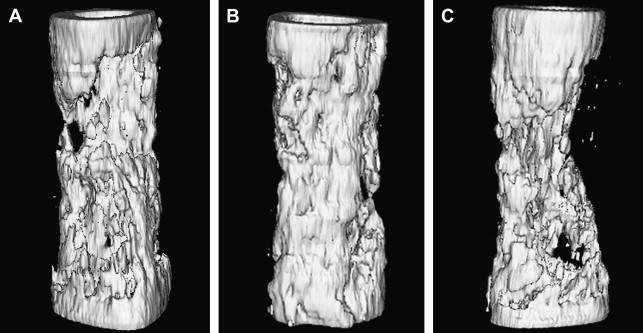
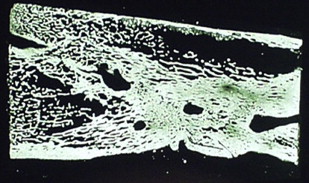
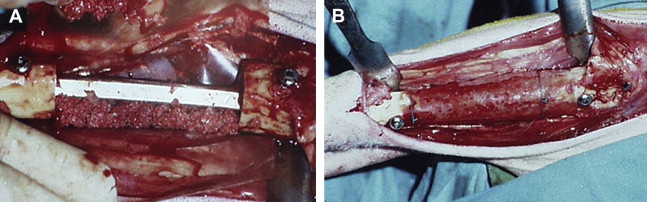
The theoretical basis for using membranes to span segmental defects was, therefore, well established by the late 1980s. Initial animal studies confirmed the potential efficacy of membranes in critical-sized diaphyseal defects. These membranes were fabricated with polylactide, which is a material with a long-established clinical history in orthopedic surgery as resorbable sutures. Microporous membranes were used as tubular stints that spanned diaphyseal defects of the rabbit radius. Membranes applied across a 1-cm segmental defect spontaneously healed with intralumenal woven bone and appositional bone formation along the outer membrane surface. Untreated defects failed to reconstitute and the defect filled with fibrous tissue and surrounding muscle ( Figs. 1 and 2 ). The basic mechanisms for enhanced bone healing with membranes was demonstrated in the rabbit model as : exclusion of nonosseous tissues, maintenance of an osteogenic medullary canal, and the provision of a spatial scaffold for periosteal regeneration and revascularization. Subsequent studies on larger defects of 2.5 to 7 cm in Yucatan minipig, goat, and sheep long bones showed that there was inconsistent spontaneous bone regeneration and that augmentation with autogenous bone graft was efficacious. In larger bone defects, revascularization from the surrounding soft tissues is a critical factor for defect healing with membranes. In addition, variables, such as membrane chemistry, resorption rates, membrane porosity, membrane thickness, and structure become increasingly important in larger defects. Numerous animal studies were performed to investigate these different membrane variables and the supplemental modes of defect stabilization, such as external fixation, locked nails, and locked plates. One of the most efficacious configurations studied was the use of two microporous (50–70 micrometer), poly (L/DL-lactide) meshed membranes (800–900 micrometer) to form a tube within a tube bridging a stabilized diaphyseal defect. The resultant space between the membranes, when grafted with autogenous bone graft, uniformly reconstituted a neocortex. The double membrane technique reduces the amount of autogenous bone needed to form a new cortical construct. In addition, bone formation was most extensive in the areas of the defect where there was an abundant muscle soft-tissue envelope. The meshed membranes were efficacious in excluding soft-tissue invasion while allowing for vascular ingrowth. In addition, the mesh construct reduces the amount of polymer material to be resorbed. Zibi fig. of membranes from Gugala and colleagues ( Figs. 3 and 4 ) .
One of the primary clinical advantages of the polylactide membrane is its bioresorption. Because it is bioresorbable and biocompatible, there is no need for additional surgical explantation. The membrane is radiolucent to permit conventional radiographic, CT, and MRI of the bone regeneration. In addition, the bioresorption eliminates any potential effects of stress shielding. The animal studies confirmed that the degradation of polylactide membranes into local lactic acid, and ultimately water and carbon dioxide, was well tolerated by the host. Numerous histologic specimens among various animal species demonstrated early incorporation of the membrane by regenerate bone without an inflammatory response ( Fig. 5 ). Membranes that were loaded with calcium carbonate (CaCO3) demonstrated the feasibility of adding bone mineral substrate for additional osteoconductive and biologic activity ( Fig. 6 ). Membranes could also be heat molded into various tubular structures or curved surfaces as needed to fit the clinical defect ( Fig. 7 ). At the conclusion of the animal studies, membrane chemical composition, porosity, and gross structure, such as thickness and meshing, had been adequately studied for the fabrication of a membrane that was suitable for human implantation. In addition, membranes had been studied with and without bone graft, with plate stabilization, intramedullary (IM) nail stabilization, and in situ for small defects. Thus, it appeared that polylactide mesh membranes, when combined with stable fixation and autogenous bone graft, would be a suitable treatment modality in the human clinical situation.
Related posts:
 Clavicle Fractures in 2010: Sling/Swathe or Open Reduction and Internal Fixation?
Viable Bone and Circulatory Factors Required for Survival of Bone Grafts
Treatment of Large Segmental Bone Defects with Reamer-Irrigator-Aspirator Bone Graft: Technique and Case Series
Autologous Bone Graft: When Shall We Add Growth Factors?
Use of the Induced Membrane Technique for Bone Tissue Engineering Purposes: Animal Studies
Soft Tissue and Biomechanical Challenges Encountered with the Management of Distal Tibia Nonunions
Clavicle Fractures in 2010: Sling/Swathe or Open Reduction and Internal Fixation?
Viable Bone and Circulatory Factors Required for Survival of Bone Grafts
Treatment of Large Segmental Bone Defects with Reamer-Irrigator-Aspirator Bone Graft: Technique and Case Series
Autologous Bone Graft: When Shall We Add Growth Factors?
Use of the Induced Membrane Technique for Bone Tissue Engineering Purposes: Animal Studies
Soft Tissue and Biomechanical Challenges Encountered with the Management of Distal Tibia Nonunions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


