Chapter 1. Clinical reasoning in orthopaedic medicine
CHAPTER CONTENTS
SUMMARY
Orthopaedic medicine is based on the life’s work of the late Dr James Cyriax (1904–1985). He developed a method of assessing the soft tissues of the musculoskeletal system, employing a process of diagnosis by selective tension, which uses passive movements to test the inert structures and resisted movements to test the contractile structures.
This chapter is divided into two parts. The first discusses ‘referred symptoms’ and includes patterns and ‘rules’ of referral of pain and other symptoms from different structures. The second, ‘clinical examination’, describes the theory behind Cyriax’s logical method of subjective and objective examination, which, by reasoned elimination, leads to the incrimination of the tissue in which the lesion lies.
REFERRED SYMPTOMS
Patients usually complain of pain but there may be other symptoms that cause them to seek advice, such as stiffness, weakness, numbness and pins and needles. Since pain is the most usual complaint, it will form the basis of this discussion.
Whether right or wrong in their assessment, patients usually localize their pain as coming from a certain point and can describe the area of its spread, although sometimes only vaguely. Cyriax considered that all pain is referred and explored the pattern of referred pain to try to establish some rules that would help in its interpretation towards establishing its true source (Cyriax & Cyriax 1993).
The study of pain itself is a vast topic, most of which is outside the scope of this book, and the reader is referred for a detailed account to the many other sources that confine themselves to the in-depth study of this field. Nevertheless, pain and its behaviour are relevant to orthopaedic medicine, particularly in the assessment procedures, both towards the achievement of an accurate clinical diagnosis and as a guide to the effectiveness of the treatment techniques applied.
To be able to identify the source of the pain, a thorough knowledge of applied and functional anatomy is essential, coupled with an understanding of the behaviour of pain, particularly in relation to its ability to be referred to areas other than the causative site. It is acknowledged that other influences can affect the perception of pain and within this chapter referred pain will be discussed, with a brief consideration of psychosocial factors.
Discussion of the possible mechanisms and patterns of referred pain
It is commonly found in clinical practice that pain of visceral origin can mimic that of somatic origin (‘pain arising from noxious stimulation of one of the musculoskeletal components of the body’, Bogduk 2005) and vice versa. Pain arising from pathology in the heart, for example, may produce a spread of pain into the arm, imitating the pain of nerve root sleeve compression from a cervical lesion. Similarly, mid-thoracic back pain may arise from a stomach lesion. Visceral pain tends to be inflammatory in origin, since the viscera are relatively insensitive to mechanical pressure, whereas somatic pain can arise from either or both causes (Lundeburg & Ekholm 2002).
There have been several suggestions put forward for the mechanism of referred pain and the more significant ones are discussed here. McMahon et al (1995) cite Sinclair who suggested that primary sensory neurons have bifurcating axons which innervate both somatic and visceral structures. Some evidence was found for this theory, but some of the findings were challenged, particularly as such axons had failed to be demonstrated in appreciable numbers. While unable to find neurons with visceral and somatic fields, McMahon et al mention that Mense and colleagues did find a few single sensory neurons with receptive fields in two tissues, in both skin and muscle in the tail of a cat, but overall there was scant support for Sinclair’s suggestion.
More recently, Sameda et al (2003) have demonstrated peripheral axons dichotomizing (branching into two) into both the L5, L6 disc and groin skin in rats. This could provide a possible explanation for pain referred to the groin area from damage to the L5 and S1 nerve roots from L4–L5 and L5–S1 disc herniation in humans, in spite of the nerve supply of the groin area arising from the higher lumbar spinal nerves.
Evidence has been provided for the mechanism that visceral and somatic primary sensory neurons converge onto common spinal neurons, causing confusion in the ascending spinal pathways and leading to misinterpretation of the origin of the pain. The message from the primary lesion could be wrongly interpreted as coming from the area of pain referral (Vecchiet & Giamberardino 1997, Robinson 2003). This has been dubbed the convergence–projection theory.
A side-track from the ‘convergence–projection theory’ is the ‘convergence–facilitation theory’, attributed to McKenzie (cited in McMahon et al 1995), which claimed that the viscera are insensitive and that visceral afferent activity does not directly give rise to pain. It was suggested that an irritable focus was produced within the spinal cord, where somatic inputs would take over to produce abnormal referred pain in the appropriate segmental distribution. This theory was not generally accepted, however, since it denied that true visceral pain could exist. However, it did provide an explanation for heightened referred sensations, including that of secondary hyperalgesia (Vecchiet & Giamberardino 1997). Its basic concepts have been developed under the descriptor of ‘central sensitization’ that explains hyperalgesia and the prolongation of chronic pain as arising from the augmented response of signalling neurons in the central nervous system as a result of inflammation or compression of nerve structures (Niere 1991, Butler 1995, Mendelson 1995, Campbell & Meyer 2006).
As mentioned above, there are no separate ascending spinal pathways for the transmission of visceral pain, and sensations from the viscera are represented within the somatosensory pathways, that also transfer sensations from somatic structures (Galea 2002). This can lead to confusion in differential diagnosis between pain arising from visceral lesions and that arising from musculoskeletal lesions. Galea describes how the level of the spinal cord to which visceral afferent fibres project depends on their embryonic innervation and notes that many viscera migrate well away from their embryonic derivation during development, such that visceral referred pain may be perceived at remote sites.
Referred pain does not only present itself for misinterpretation between visceral and somatic structures but is also a phenomenon which may prevent accurate localization among the musculoskeletal tissues. Cyriax & Cyriax (1993) suggested that the misinterpretation of pain occurs at cortical level where stimuli arriving at certain cortical cells from the skin can be localized accurately to that area. When stimuli from other deeper tissues of the same segmental derivation reach those same cells, the sensory cortex makes assumptions on the basis of past experience and attributes the source of the pain to that same area of skin. This accounts for the dermatomal reference of pain but the theory can be extended to include the referral of other symptoms from structures within the same segment.
SEGMENTAL REFERENCE
Knowledge of the nerve supply of soft tissue structures, coupled with factors affecting segmental reference and the general rules of referred pain, is a useful aid to diagnosis. It will help to direct the clinician to the true source of the patient’s pain and so facilitate the application of effective treatment.
Several workers have tried to establish patterns of referred pain by examining the dermatomes. However, the dermatomes appear to vary according to the different methods for defining them. These mainly derive from embryonic development, observation of herpetic eruptions, areas of vasodilatation resulting from nerve root stimulation and the areas of tactile sensation remaining after rhizotomy (surgical severance) of spinal nerve roots, as described below. These dermatomes are referred to as embryonic, herpetic, vasodilatation and tactile, respectively.
Sir Henry Head (1900) laid the foundations for the mapping of dermatomes by analysing herpetic eruptions. Herpes zoster is an inflammatory lesion of the spinal ganglia which produces an eruption on the skin in the corresponding segmental cutaneous area. By defining the dermatomes in this way, little overlap was found and there was only slight variation between subjects studied.
Stricker & Bayliss, as described by Foerster (1933), used faradic stimulation of the distal part of a divided posterior root to produce vasodilatation. This produced a clearly defined area similar to the dermatomes defined in the isolation method, but slightly smaller in size.
The skin is supplied by both ventral and dorsal nerve roots. Foerster (1933) examined the areas of skin supplied by the dorsal roots which carry the afferent sensory fibres and efferent fibres producing vasodilatation. He described two methods of isolating the area of skin supplied by the dorsal nerve roots, using the terms ‘anatomical’ and ‘physiological’.
The anatomical method, attributed to Herringham & Bolk (Foerster 1933), involved the isolation of fibres arising from a single nerve root by dissection through the plexus and the peripheral nerves into the skin. It was impossible to follow the finest ramifications by this method but it largely demonstrated that there was little or no overlap of dermatomes classified in this way.
Within the physiological method of differentiation, Foerster (1933) describes how Sherrington divided the nerve roots above and below a single nerve root to map the area supplied by the intervening intact root in the monkey. There was such overlap of different dermatomes identified by this method that division of a single root produced no loss of sensibility. He used the same technique in humans and found the same pattern of overlap in the tactile dermatomes.
Lee et al (2008) set out to produce a novel dermatome map based on the available evidence drawn from experiments conducted over the past century (Fig. 1.1) They proposed that the overlapping of dermatomes and their variability deserved more emphasis and that to represent dermatomes as autonomous zones of cutaneous sensory innervation is unreliable.
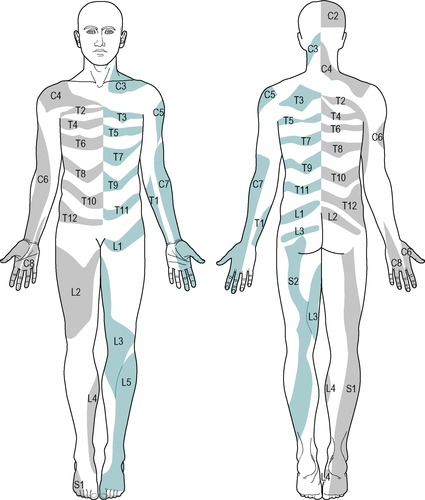 |
| Figure 1.1 The evidence-based dermatome map representing the most consistent tactile dermatomal areas for each spinal dorsal nerve root found in most individuals, based on the best available evidence. The dermatomal areas shown are NOT autonomous zones of cutaneous sensory innervation since, except in the midline where overlap is minimal, adjacent dermatomes overlap to a large and variable extent. Blank regions indicate areas of major variability and overlap. S3, S4 and S5 supply the perineum but are not shown for reasons of clarity. From Lee M W L, McPhee R W, Stringer M D 2008 An evidence-based approach to human dermatomes. Clinical Anatomy 21:363–373. Reprinted with permission of John Wiley & Sons, Inc. |
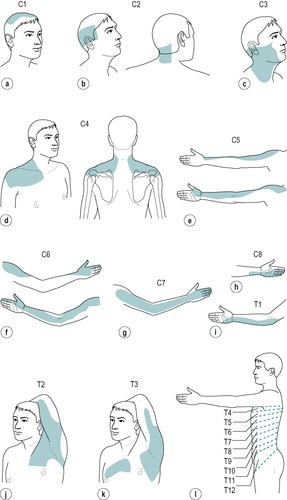
However, despite the experimental findings, the extent of individual dermatomes, especially in the limbs, is largely based on clinical evidence and Standring (2009) acknowledged that this leads to a wide variation between the opinions of different disciplines. The dermatomes given in this book are drawn mainly from the clinical experience of Cyriax and are different from those given in Gray’s Anatomy (Standring 2009), for example. In the authors’ experience, they provide a basic guide for clinical practice and are presented as shown in Figure 1.2.
 |
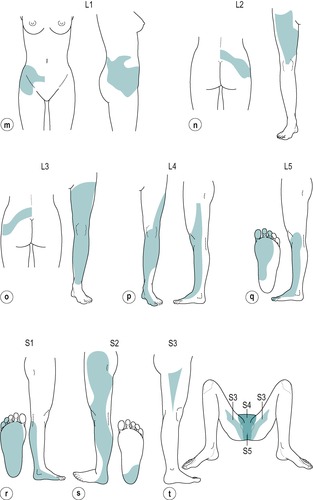 |
| Figure 1.2 Dermatomes. C1: top of head (Fig. 1.2a) C2: side and back of the head, upper half of the ear, cheek and upper lip, nape of the neck (Fig. 1.2b) C3: entire neck, lower mandible, chin, lower half of the ear (Fig. 1.2c) C4: epaulette area of the shoulder (Fig. 1.2d) C5: anterolateral aspect of the arm and forearm as far as the base of the thumb (Fig. 1.2e) C6: anterolateral aspect of the arm and forearm, thenar eminence, thumb and index finger (Fig. 1.2f) C7: posterior aspect of the arm and forearm, index, middle and ring fingers (Fig. 1.2g) C8: medial aspect of the forearm, medial half of the hand, middle, ring and little fingers (Fig. 1.2h) T1: medial aspect of the forearm, upper boundary uncertain (Fig. 1.2i) T2: Y-shaped dermatome, medial condyle of humerus to axilla, branch to sternum and branch to scapula (Fig. 1.2j) T3: area at front of chest, patch in axilla (Fig. 1.2k) T4, 5, 6: circling trunk above, at and below the nipple area (Fig. 1.2l) T7, 8: circling trunk at lower costal margin (Fig. 1.2l) T9, 10, 11: circling the trunk, reaching the level of the umbilicus (Fig. 1.2l) T12: margins uncertain, extends into groin, covers greater trochanter and the iliac crest (Fig. 1.2l) L1: lower abdomen and groin, lumbar region between levels L2 and L4, upper, outer aspect of the buttock (Fig. 1.2m) L2: two separate areas: lower lumbar region and upper buttock, whole of the front of the thigh (Fig. 1.2n) L3: two separate areas: upper buttock, medial aspect and front of the thigh and leg as far as the medial malleolus (Fig. 1.2o) L4: lateral aspect of the thigh, front of the leg crossing to the medial aspect of the foot, big toe only (Fig. 1.2p) L5: lateral aspect of the leg, dorsum of the whole foot, first, second and third toes, inner half of the sole of the foot (Fig. 1.2q) S1: sole of the foot, lateral two toes, lower half of the posterior aspect of the leg (Fig. 1.2r) S2: posterior aspect of the whole thigh and leg, plantar aspect of the heel (Fig. 1.2s) S3: circular area around the anus, medial aspect of the thigh (Fig. 1.2t) S4: saddle area: anus, perineum, genitals, medial upper thigh (Fig. 1.2t) S5: coccygeal area (Fig. 1.2t) |
Nerve root dermatomes
In general the muscle groups lie under the dermatome which shares the same nerve supply. However, the dermatome and myotome may not overlie each other and there are some apparent exceptions to this rule. This can cause confusion in the consideration of referred pain, in that a lesion in the relevant muscle may appear to refer pain to an unrelated site and vice versa.
As mentioned above, the viscera may also refer pain to apparently unrelated sites and this should also be considered within differential diagnosis. Pappano & Bass (2006) present a case study describing referred shoulder pain preceding abdominal pain in a teenage girl with gastric perforation. The paper also highlights other conditions as referring to the shoulder including peritonitis, cholecystitis and subdiaphragmatic endometriosis. Post-laparoscopy shoulder pain is noted, where carbon dioxide used for inflation applies stretch to the diaphragm. Sloan (2008) provides further detail listing right-sided periscapular pain in gall bladder disease and interscapular pain in aortic dissection.
The most commonly encountered discrepancies are as follows:
• Scapular muscles are supplied by C4–C7, but underlie thoracic dermatomes
• Latissimus dorsi is supplied by C6–C8, but underlies thoracic and lumbar dermatomes
• Pectoralis major is supplied by C5–T1 but underlies thoracic dermatomes
• The heart, a thoracic structure, is supplied by C8–T4 and may refer pain into the arm, axilla and chest
• The diaphragm is supplied by C3–C5 and diaphragmatic irritation may lead to pain being felt in the epaulette region of the shoulder
• The gluteal muscles are supplied by L5, S1–S2 but underlie L1–L3 dermatomes
• The testicle is supplied by T11–T12, but underlies the S4 dermatome where pain may be felt locally or can be referred to the lower thoracic or upper lumbar regions.
Cyriax (1982) and Cyriax & Cyriax (1993) identified several factors that influence the referral of pain:
• Strength of the stimulus
• Position of the structure in the dermatome
• Depth of the structure
• Type or nature of the structure.
Strength of the stimulus
The more acutely inflamed or irritable the lesion (i.e. the greater the stimulus), the further into the dermatome will the symptoms be referred (Inman & Saunders 1944). For example, an acutely inflamed subacromial bursitis may refer its pain to the wrist, the distal extent of the C5 dermatome, and a lumbar lesion involving compression and inflammation of the L4 nerve root may refer pain and associated symptoms to the big toe, at the distal end of the L4 dermatome.
Position in the dermatome
Pain and tenderness tend to refer distally. Therefore a structure placed more proximally in the dermatome is capable of referring its symptoms over a greater distance to the end of the dermatome.
The length or distance of dermatomal referral is particularly obvious in the limbs, where the dermatomes tend to be long. However, if the dermatome is short, even with an acutely inflamed or irritable lesion, the reference will halt at the end of its dermatome, or the most distal dermatome in the event of more than one nerve supply.
Structures within the hand and forefoot are already at the distal end of their relevant dermatome. Referral of symptoms is therefore less and such lesions are easier to localize (Inman & Saunders 1944).
Depth of the structure
Skin is the only organ that provides precise localization of pain and is of course the most superficial structure (Gnatz 1991). Cyriax (1982) proposed that lesions in the more deeply placed structures tend to give greater reference of pain, which was also the finding of Kellgren (1939) and Inman & Saunders (1944). The deeper structures therefore give rise to greater misunderstanding in terms of clinical diagnosis.
Joint, ligament (e.g. medial collateral and anterior cruciate ligaments) and bursa lesions tend to conform to this assumption but a notable exception is provided by lesions within bone. Pain and tenderness arising from fractures or involvement of the cortical bone tend to be well localized, even though bone itself is the most deeply placed tissue in musculoskeletal terms. Lesions involving the cancellous part of bone may give the more typical pattern of referred pain.
Segmental pain arising from lesions in the deeply sited viscera can also be misleading.
Nature of the tissue
The factor of depth of the structure should perhaps be considered alongside that of the nature of the tissue, since studies to observe the effect of lesions in tissues of different nature and site on patterns of referred pain are hard to dissociate.
Kellgren (1938, 1939) observed patterns of referred pain induced by the injection of 6% hypertonic saline into deeply placed structures including muscle, tendon sheaths, fascia, periosteum and interspinous ligaments. On injection of muscle, diffuse referred pain was produced which appeared to follow a segmental pattern and was associated with deep tenderness rather than hyperaesthetic skin. Witting et al (2000) compared local and referred pain following intramuscular capsaicin injection into the brachioradialis muscle and intradermal injection in the skin above the muscle. Intradermal injection produced more intense but localized pain whereas referred pain was more marked after the intramuscular injection and was deeply located as well as referring to skin.
Kellgren also observed that pain arising from the limb muscles tended to refer to the region of the joints moved by these muscles, where it could easily be confused as arising from the joint itself. Farasyn (2007) adds support to the observation that muscles refer pain, describing that a local muscle lesion can give rise to a wider area of pain, separate from the tender local injury and often described as ‘burning’.
Tendon sheath and fascia gave sharply localized pain. Stimuli did not produce pain from articular cartilage or compact bone but when applied to cancellous bone a deep diffuse pain was produced. Stimulation of the interspinous ligaments gave rise to segmentally referred pain which, as in muscle, was associated with tenderness in the deeply placed structures.
Inman & Saunders (1944) noted a variability of sensitivity of the different structures beneath the skin, creating a ‘league table’ of those tissues with the highest sensitivity to those with the least, as follows: bone, ligaments, fibrous capsules of joints, tendons, fascia and muscle. These findings were supported in part by Kuslich et al (1991), who investigated tissues in the lumbar spine as potential sources of low back pain using progressive local anaesthetic during exploratory operation of the spine. Their emphasis too was that muscles, fascia and the periosteum and compact layer of bone (they did not test cancellous bone) were relatively insensitive. In contrast, in the work of Travell & Simons (1996) trigger points in muscle have been identified as a focus of hyperirritability which gives rise to local tenderness and referred pain.
It had been particularly noted by Inman & Saunders (1944) that capsules and ligaments were most sensitive close to their bony attachments, and therefore most likely to be pain-producing following trauma to these commonly injured sites.
Controversy has existed for many years as to whether the disc or the zygapophyseal joint is the primary source of back pain, especially when associated with pain in the limb. Aprill et al (1989) studied the reference of pain from the cervical zygapophyseal joints to establish whether each joint had a specific area of reference of pain in a segmental distribution. They found reasonably distinct and consistent segmental patterns of pain referral associated with joints between each of the levels of C2–C7, but there was no referral of pain into the arm from any of the tested levels. The paper acknowledged that the study had not set out to distinguish the pain arising from zygapophyseal joints from other potential sources.
In support of this pattern of referral, Cooper et al (2007) set out to determine the patterns of referred pain arising from cervical zygapophyseal joints by using diagnostic blocks to establish pain referral patterns in symptomatic subjects. There was considerable overlap of referral areas and patients described the symptoms in lines, spots or patches that were mostly confined to the neck and shoulder region. They reported some variation from the results of their previous studies conducted on non-symptomatic subjects and suggested that the outcome might be due to the length of time that patients had been experiencing symptoms.
Maintaining the emphasis on the nature of the tissue, two pain syndromes of somatic and radicular origin have been described associated with the spinal joints (Bogduk 2005). In somatic pain syndromes it is proposed that the source of the pain could be in any structure in the spine that receives a nerve supply, i.e. muscles, ligaments, zygapo-physeal joints, intervertebral discs, dura mater and dural nerve root sleeve. Somatic pain is not associated with neurological abnormalities and does not involve nerve root compression. The quality of somatic pain is described as dull, diffuse and difficult to localize.
For clarity, ‘ somatic pain’ is distinct from ‘ visceral pain’ where the noxious stimulation occurs within an organ. It is also distinct from ‘ neurogenic pain’ where the nociceptive information arises as a result of irritation or damage to the axons or cell bodies of a peripheral nerve, not to the nerve endings (Bogduk 2005).
A further distinction should be made between ‘ radiculopathy’ and ‘ radicular pain’.
Radiculopathy is a neurological condition where conduction is blocked in the axons of a spinal nerve or its roots. Conduction block in sensory axons results in numbness, and conduction block in motor axons results in weakness. Radiculopathy is a state of neurological loss and it does not result in pain, either in the back or limbs. However it may, or may not, be associated with radicular pain. The aetiology (cause) of both can be the same but the mechanisms are different.
In radicular pain syndromes, the radicular (root) pain arises as a result of irritation of a spinal nerve or its roots. Contrary to the traditional belief, it is not caused by compression or traction of nerve roots, unless the nerve root has become sensitized by previous damage (Kuslich et al 1991). Robinson (2003) confirmed this by stating that an inflammatory component or already damaged nerve root is necessary before a nerve root will produce pain.
Radicular pain occurs as the result of compression of dorsal root ganglia when activity occurs not only in nociceptive axons but also in A-beta fibres (Niere 1991, Bogduk 2005). Disc herniation is the most common cause of radicular pain. However, as well as compression of the dorsal root ganglion, from anatomical abnormalities, leakage of inflammatory mediators from the nucleus pulposus into the epidural space has also been proposed as a cause of radicular pain (Peng et al 2007). Both mechanisms may result in an inflammatory reaction causing hyperexcitability and spontaneous ectopic activity in the dorsal root ganglion, which is interpreted as pain. This can also add to central sensitization at the dorsal horn synapses (Niere 1991).
As discussed above, experimental compression of dorsal root ganglia or previously damaged nerve root has been shown to cause radicular pain. The clinical experiments of Smyth & Wright show this pain to be produced in a particular form, namely lancinating and shooting in quality, and referred in relatively narrow bands (Smyth Wright 1959, Bogduk 2005). Taking into account the overlapping nature of somatic and radicular pain referral patterns, Robinson (2003) suggests that the patient’s description of the pain itself may be more reliable than the location. Table 1.1 attempts to draw out the key differences between somatic and radicular pain, based on subjective and objective descriptors, to aid clinical reasoning and diagnosis.
| SOMATIC PAIN | RADICULAR PAIN | |
|---|---|---|
| Source of pain? | A deep musculoskeletal structure, e.g. dural nerve root sleeve, muscle, zygapophyseal joint, with a nerve supply from a specific segment. | Pain deriving from damage or irritation of the spinal nerve tissue, particularly the dorsal root ganglion. |
| Pain is referred where? | Segmentally referred dermatomal pain according to the nerve supply of the structure. | Segmental reference, more commonly to distal end of dermatome in limb (little back pain). |
| Pain is described as? | Deep ache, vague, poorly localized. | Lancinating, burning, severe, radiating, deep, strap-like, narrow, well localized, may be latent in nature. |
| Is there any neurology? | None associated. Nociceptive stimulation of somatic structures will not produce any neurological signs. | Yes. Usually associated with radiculopathy giving paraesthesia, numbness, muscle weakness and reduced reflexes in the appropriate segment. |
| Clinical tips | Somatic pain can precede, and often be associated with, radicular pain since the dural nerve sleeve is a somatic structure surrounding the spinal nerve root. | Once chronic, radicular pain becomes more difficult to differentiate from somatic pain due to central sensitization, i.e. increased excitability of pain-related central nervous system neurons and the widening out of the pain field. |
Bogduk (1994) proposed that somatic and radicular pain syndromes can coexist. For example, the annulus fibrosus of the disc may be a source of somatic low back pain but may also cause secondary compression by a posterolateral displacement causing compression of the nerve root leading to radicular pain. However, a lesion cannot selectively compress nociceptive axons; therefore, for compression to be the source of radicular pain, other neurological abnormalities associated with radiculopathy should be present, e.g. paraesthesia, numbness, muscle weakness and loss of reflexes (Bogduk 2005).
Kidd & Richardson (2002) further clarify that somatic referred pain is nociceptive, being initiated by stimulation of receptors on peripheral terminals of sensory fibres, by either damage or inflammation within somatic structures. In contrast, radicular pain is neuropathic and arises as a result of sensory fibres being abnormally stimulated along their course.
Grieve (1981) observed that ‘all root pain is referred pain, but not all referred pain is root pain’. Kellgren (1939), in charting the distribution of pain, demonstrated that injection of the interspinous ligaments of L2–S2 produced pain in the leg. However, as referred to above, Kuslich et al (1991) found that sciatica could only be produced by stretching or direct pressure on an already inflamed nerve root.
In Kuslich’s study, the zygapophyseal joint capsule was found to be tender in some instances but the pain was never referred to the leg. The zygapophyseal joint’s main significance in the production of low back pain was its ability to compress or irritate other local sensitive tissues, particularly with osteophyte formation, including the annulus fibrosus. The annulus fibrosus was demonstrated to be the tissue of origin in most cases of low back pain without pain or symptom referral into the limb. It should be noted that the sacroiliac joint was not included in either study to be able to establish its ability to produce leg pain.
O’Neill et al (2002) demonstrated that noxious stimulation of the intervertebral disc can give rise to low back and referred extremity pain, with the distal extent of pain produced depending on the intensity of stimulation. Nociceptors within the discal tissue may have become more sensitized in patients presenting with non-radicular leg pain allowing provocation of peripheral symptoms at lower thresholds of stimulation. They suggest that Kuslich et al (1991), discussed above, would have observed a similar pattern of pain referral on stimulation of the annulus, and other structures, if they had applied a stimulus of sufficient intensity.
O’Neill et al support Bogduk (2005) in describing referred leg pain from the somatic lumbar annulus fibrosus as being poorly localized, dull and aching, adding that it is usually less troublesome than the patient’s low back pain. They warn that it is important to be able to differentiate between referred pain arising from somatic structures and radicular pain associated with nerve root compression from disc herniation, because the two types of pain have different causal mechanisms and may therefore require different treatment. They add that the traditional description ‘pain radiating below the knee’ as representing radicular pain rather than referred somatic pain is unreliable.
As mentioned above Bogduk (2005) claims that for referred leg pain to be radicular in origin, arising from compression of a nerve root, it must be accompanied by other signs of compression – paraesthesia and muscle weakness. If these are absent, pain referred to the limb must be somatic in origin.
Schäfer et al (2009) have attempted to classify the causal mechanisms of leg pain into four groups that may help to guide treatment approaches, although they acknowledge that there is likely be some overlap. As well as radicular pain with motor loss and musculoskeletal (somatic) causes, they propose that leg pain can also arise from central and peripheral nerve sensitization.
Within this text, specific consideration of visceral referred pain is provided within the appropriate chapters as part of differential diagnosis. However, just as we have attempted to separate out the characteristics of somatic and radicular pain, Vecchiet & Giamberardino (1997)




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
