Clinical Pathways Following Total Hip Replacement
Andrew Freiberg
Lauren Lebrun
Gregory Pauly
Introduction
Clinical pathways are standardized care management protocols that extend over a defined episode of care. Clinical pathways are synonymous with practice guidelines, clinical protocols, clinical algorithms, and care process models (1). Pathways serve as a tool to (1,2)
translate national guidelines and best practices into local protocols
organize and sequence the actions of interdisciplinary care teams
reduce variation in practice as a mechanism to improve outcomes
facilitate appropriate use of resources and control costs
improve patient safety, and satisfaction
In this chapter we explore the importance of clinical pathways in arthroplasty, the development and application of standardized care protocols, and potential barriers to implementation.
Background
Clinical pathways represent the fusion of evidence-based clinical practices and systems engineering. Clinical pathways were first developed in the United States in the 1980s to control costs and improve hospital efficiencies in an environment moving toward capitated payment systems (1). Focusing on concepts of productivity and standardization, Intermountain Healthcare became known as one of the early adopters of clinical pathways. By 1995, Intermountain developed and integrated 65 pathways into clinical practice, significantly improving patient outcomes and producing a net savings of $20 million per year (3). Following suit in the early 2000s, Virginia Mason Medical Center devised a new vision and strategic plan grounded in Toyota production methodologies of waste elimination and standardization. A cornerstone of the plan was to adopt clinical pathways, internally termed as “bundles,” built upon evidence-based interventions published in the medical literature (4).
Recognizing the benefits of clinical pathways and care improvement programs, many hospitals and health systems have adopted principles employed by Intermountain Healthcare and Virginia Mason Medical Center. This has largely been fueled by changes in reimbursement shifting financial risk from insurers and employers to patients and providers. Many insurance plans steer patients to low-cost facilities. For example, through reference pricing the insurer pays a defined contribution towards a hospital bill and the patient is responsible for paying the remainder, influencing the patient to shop for the lowest priced care (5). Similarly through centers-of-excellence contracting, insurers and employers restrict or drive patients to specific hospitals deemed by the insurer as providing high-quality and low-cost care (5). Providers are also at financial risk for the efficiency and outcomes of the care they provide under risk arrangements such as accountable care organizations, bundled payments, and pay-for-performance programs (5,6).
Risk arrangements, tied to both cost and quality outcomes, highlight the importance of efficient, patient-centered and quality-driven clinical pathways for physicians and hospitals to remain competitive in the current marketplace. In joint replacement, outcomes research has shown that adherence to evidence-based guidelines can have a greater impact on procedural outcomes than surgeon and hospital volumes (7). Moreover, the one-on-one surgeon-to-patient relationship has evolved, and patient care teams can now involve upward of 60 people, requiring intensive coordination and teamwork across multiple disciplines (8). These factors, coupled with a projected 174% increase in the US demand for total hip replacement procedures and 673% increase for total knee replacement procedures by 2030, underscore the necessity of clinical pathways in arthroplasty (9).
Overview of Arthroplasty Pathways
There are more than 500 arthroplasty pathways published in orthopedic and healthcare management literature (10). There is however no standard definition of what constitutes a clinical pathway, and publications describe a wide array of pathway types from simplistic to sophisticated models (2).
On a simplistic level, the adherence to process-of-care measures grounded in evidence-based practice defines the
foundation of a clinical pathway. In their research, Bozic et al. studied compliance with four process measures—use of prophylactic antibiotics on the day of surgery, continuation of antibiotics 24 hours postsurgery, use of beta blockers in the first 2 days postsurgery in patients at high risk for perioperative myocardial infarction, and use of venous thromboembolism prevention in the first 2 days postsurgery—and the impact on patient outcomes in total joint replacement. Their findings showed that missed process-of-care measures increased the risk of negative outcomes including readmission, reoperation, complications, and increased length of stay (10).
foundation of a clinical pathway. In their research, Bozic et al. studied compliance with four process measures—use of prophylactic antibiotics on the day of surgery, continuation of antibiotics 24 hours postsurgery, use of beta blockers in the first 2 days postsurgery in patients at high risk for perioperative myocardial infarction, and use of venous thromboembolism prevention in the first 2 days postsurgery—and the impact on patient outcomes in total joint replacement. Their findings showed that missed process-of-care measures increased the risk of negative outcomes including readmission, reoperation, complications, and increased length of stay (10).
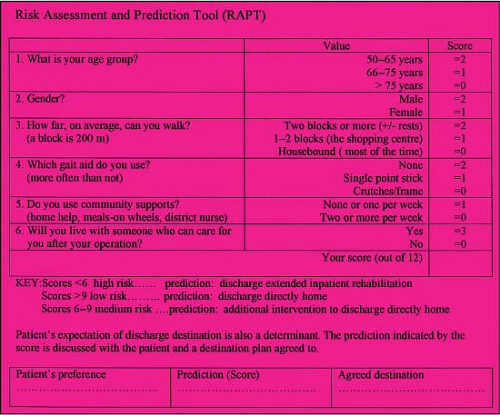 Figure 34.1. Risk Assessment and Prediction Tool (RAPT). (Reprinted with permission from Oldmeadow LB1, McBurney H, Robertson VJ. Predicting risk of extended inpatient rehabilitation after hip or knee arthroplasty. J Arthroplasty. 2003;18(6):775–779.) |
On a sophisticated level, many hospitals and health systems utilize clinical pathways as a “playbook.” The tasks of all care team members—surgeons, anesthesiologists, case managers, nurses, physical therapists, occupational therapists, and others—are clearly defined and organized from preadmission to postdischarge. Examples of two such pathways in arthroplasty, both universal for hip and knee replacement procedures, are described in the following sections.
Massachusetts General Hospital Arthroplasty Pathway
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


