Casting for Early-Onset Scoliosis
James O. Sanders
DEFINITION
Early-onset scoliosis is defined as scoliosis occurring by age 5 years. The term was developed because it is more likely associated with long-term pulmonary compromise than in children with later onset scoliosis.2, 16
Infantile scoliosis is another term referring to scoliosis detected by age 3 years. It usually refers to idiopathic scoliosis unlike “early-onset scoliosis” which can include congenital and neuromuscular curves. Occasionally, the term infantile scoliosis will include syndromic children because of the difficulty in identifying many syndromes in young children. Practically, infantile and early-onset scoliosis are often used synonymously.
ANATOMY
Infantile scoliosis is a deformity of the discs, vertebral bodies, and the chest wall. The ribs articulate with the vertebra at both the transverse processes (costotransverse joints) and the vertebral bodies (costovertebral joints).
The spine is usually rotated about the longitudinal axis with the lateral convex side more posterior than the concave side (FIG 1).
PATHOGENESIS
The pathogenesis of idiopathic or most syndromic early-onset scoliosis is unknown. Early-onset scoliosis may have an underlying neurologic or muscular abnormality.
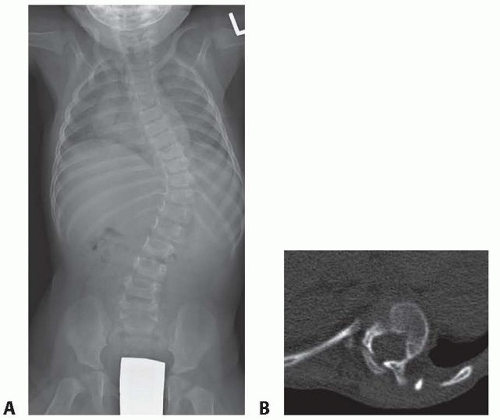
FIG 1 • A. An AP radiograph of a 12-month-old child with a typical left lower thoracic infantile scoliosis. B. A computed tomography (CT) scan at the apex of an infantile scoliosis showing the rotation with the anterior spine rotated toward the concavity and the posterior spine toward the convexity.
NATURAL HISTORY
Infantile curves may be either resolving or progressive with resolving curves being far more common.
Scoliosis presenting during the first year of life has a greater likelihood of resolving spontaneously, whereas curves developing after 1 year of age have a worse prognosis.12, 13
Both the rib-vertebral angle difference (RVAD) and rib phase are important for predicting which curves will progress15 (FIG 2).
The RVAD is the difference of the angles made between each rib and the corresponding vertebral body. This is measured at the vertebral level with the greatest angular difference between the concave and convex rib.
Rib phase is classified as phase 1 or 2, depending on whether or not spinal rotation causes the rib head to overlap the vertebral body (phase 1, no overlap; phase 2, overlap).
Eighty-three percent of resolving curves have a RVAD of less than 20 degrees and 83% of progressing curves have a RVAD of greater than 20 degrees.
In progressive curves, the RVAD increases and the phase gradually transitions from 1 to 2.
Phase 2 ribs are the hallmark of progressive curves, as all phase 2 curves progress.
Double curves present a special problem as most of them progress.
The RVAD in double curves may be quite low, but an oblique 11th or 12th convex rib with lumbar rotation is a poor prognostic sign.
Generally, the RVAD and phase are reliable, but the measurement error may make discernment difficult in marginal cases,4 in which case, close observation, typically with repeat radiographs in 3 months, is the best course.
Left untreated, the prognosis for curves that do progress is invariably poor: By age 5 years, 57% of untreated children
will have a curve greater than 70 degrees.15 These large thoracic curves can cause restrictive lung disease or thoracic insufficiency syndrome (TIS) characterized by decreased thoracic growth and lung volume, inhibiting alveolar development and lung function, which may cause respiratory failure and death at an early age.7 The thoracic deformity can also lead to pulmonary hypertension and cor pulmonale, with respiratory failure and death occurring at a later age.3, 10, 15, 18 Curves of greater than 70 degrees are sufficient to cause cor pulmonale and have a higher mortality rate than smaller curves.10, 16
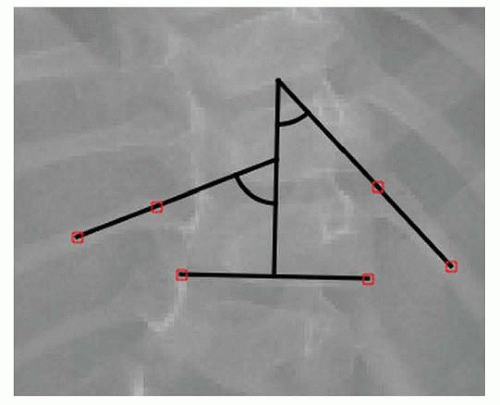
FIG 2 • The RVAD from the same child shown in FIG 1A.
Patients with progressive curves progress by about 5 degrees per year reaching 70 degrees or more by age 10 years.9, 17 Thoracic curves greater than 70 degrees in adolescence are associated with significantly lower forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) values compared to patients with smaller deformities.
EOS patients have greater pulmonary function test (PFT) impairment than adolescent idiopathic scoliosis patients.11
PATIENT HISTORY AND PHYSICAL FINDINGS
Typically, parents have noticed the deformity before their physicians. It is important to ask about a family history of nerve or muscle disorders. Unlike adolescent scoliosis, early-onset scoliosis is not often familial except in neuromuscular disorders. Because young children cannot cooperate with a manual motor examination or an Adams forward bend test, one must rely on close observation to identify the curve and any evidence of neurologic issues or myopathies.
The neurologic examination should include an assessment of gait, upper and lower extremity motor strength where feasible, tone, deep tendon reflexes including abdominal reflexes, clonus, Hoffman, and Babinski signs. Foot deformities, particularly any equinus, cavus, varus, or foot size difference may be the only neurologic signs seen.
Common syndromes associated with early-onset scoliosis include Marfan syndrome, characterized by arachnodactyly (FIG 3) and often having more severe aortic involvement in young children, and Ehlers-Danlos syndrome, characterized by marked ligamentous laxity.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


