I. MATERIALS AND EQUIPMENT
A. Plaster
- Plaster bandages and splints are made by impregnating crinoline with plaster of paris [(CaSO4)2H2O].1,2 When this material is dipped into water, the powdery plaster of paris is transformed into a solid crystalline form of gypsum, and heat is given off:

- The amount of heat given off is determined by the amount of plaster applied and the temperature of the water.3,4 The more plaster and the hotter the water, the more heat is generated. The interlocking of the crystals formed is essential to the strength and rigidity of the cast. Motion during the critical setting period interferes with this interlocking process and reduces the ultimate strength by as much as 77%. The interlocking of crystals (the critical setting period) begins, when the plaster reaches the thick creamy stage, becomes a little rubbery, and starts losing its wet, shiny appearance. Cast drying occurs by the evaporation of the water not required for crystallization. The evaporation from the cast surface is influenced by air temperature, humidity, and circulation about the cast. Thick casts take longer to dry than thin ones. Strength increases as drying occurs.
- Plaster is available as bandage rolls in widths of 8 in, 6 in, 3 in, and 2 in and splints in 5-× 45-in, 5-× 30-in, 4-× 15-in, and 3-× 15-in sizes. Additives are used to alter the setting time; three variations are available: (1) Extra fast setting takes 2 to 4 minutes, (2) fast setting takes 5 to 6 minutes, and (3) slow setting takes 10 to 18 minutes.
B. Fiberglass cast. Two decades ago, a number of companies developed materials to replace plaster of paris as a cast material. Most of these are a fiberglass fabric impregnated with polyurethane resin. The prepolymer is methylene bisphenyl diisolynate, which is converted to a nontoxic polymeric urea substitute. The exothermic reaction does not place the patient’s skin at risk for thermal injury.2,5,6 These materials are preferred for most orthopaedic applications except in acute fractures in which reduction maintenance is critical. Fiberglass casts provide lower skin pressure when compared with plaster casts when properly applied.7
- Advantages. These materials are strong and lightweight, and resist breakdown in water; they are also available in multiple colors and patterns.
- Disadvantages. They are harder to contour than plaster of paris, and the polyurethane may irritate the skin. Fiberglass is harder to apply, although the more recently introduced bias stretch material is an improvement. Review in detail the instructions from each manufacturer before using the casting materials. Patients are commonly under the impression that fiberglass casts can be gotten wet. This is incorrect; if submerged, they need to be changed to avoid significant skin maceration. Gore-Tex padding material is available to aid in drying of the material, but submersion of a cast is still to be discouraged.
C. The water. Warm water causes more heat to be given off and affords faster setting. Cold water allows for less heat and for slower setting. Plaster of paris in the water bucket from previously dipped plaster accelerates the setting time of the next plaster cast or splint. The water used for dipping should be deep enough to cover the material rolls standing on end.
D. Cast padding
- Webril has a smooth surface and less tendency for motion within the thickness of the padding than some of the other padding materials. It requires the most practice to achieve a smooth application, however.
- Specialist is softer than Webril and contains wood fiber. It has a corrugated appearance, and there is more tendency for sliding to occur within the material. It is easier to apply without wrinkles than Webril, but it becomes very hard if caked with blood.
- Sof-Roll is a soft padding similar in appearance to Webril but slightly thicker. It has greater tear resistance and is therefore easier to stretch.
- Stockinet
a. Bias-cut stockinet may be used under a cast as a single layer. It is easy to apply without wrinkles and is better than tubular stockinet if there is a large difference in the maximum and minimum diameters of the extremity. Bias-cut stockinet can be made snug throughout, in contrast to tubular stockinet, which can be snug in the large diameter of the extremity but very loose in the narrow diameter. Plaster sticks to the stockinet, so there is no sliding between the cast and the stockinet padding.
b. Tubular stockinet is made of the same material as the bias-cut type and is available in varying tube sizes from 2 in to 12 in.
- Felt or Reston should be used to pad bony prominences and for cast margins. When padding over bony prominences, such as the anterior superior iliac spine, make a cruciate incision in the felt for better contouring.
- Moleskin adhesive can be used to trim cast margins.
E. Adherent materials. Adherent substances (such as Dow Corning medical adhesive B) are applied to prevent slipping and chafing between the skin and the padding. They can contribute, however, to an increased amount of itching inside the cast. Tincture of benzoin compound should not be used in this situation because of fairly frequent skin reactions. Commercial adhesive removers are available.
F. Equipment
- Use a clean bucket. Plaster residue and other particles in the water can alter the setting time.
- Gloves keep hands clean and prevent dry skin if one applies many casts. They also make a smoother finish than is achieved by bare hands. They are mandatory for working with fiberglass materials.
- Shoe covers and aprons or gowns keep shoes and clothes clean to prevent one from appearing sloppy in plaster-covered attire.
- Use appropriate draping to maintain the dignity of the patient as well as to keep plaster off all areas not casted.
- Cast cutters
a. The cast-cutting electric saw has an oscillating circular blade that cuts firm rigid surfaces, such as casts or bony prominences. When lightly touched, the skin vibrates with the blade, but the blade does not cut. If the blade is firmly pressed against the skin or dragged along it, then it will cut. The saw is noisy and causes considerable anxiety, especially in children. Therefore, it is wise to show younger patients that cast saws are safe by touching the blade to the palm of the hand. Playing music in the cast room has been shown to decrease anxiety in children having casts removed.8 The cast saw causes dust to fly; consequently, use of this tool is best avoided in clean operating rooms. In addition, cast saws can cut skin if applied with excessive force, so it is unwise to use them on anesthetized patients.
b. Hand cutters are useful when a saw is not available or to avoid frightening a child with the noise of the saw, to lessen the amount of plaster dust in the operating room, and to remove damp plaster.
6. Cast spreaders are used to open the cut edges of a cast for access to underlying cast padding, which is then cut with scissors. Spreaders come in various sizes for large and small casts.
7. Cast knives have sharp blades and preferably have large handles for better control. Sharp blades are essential; therefore, most practitioners prefer to use no. 22 disposable surgical blades.
8. Cast benders adjust cast edges to relieve skin binding and pressure.
9. Cast dryers blow warm to hot air around a plaster cast. They are generally not necessary. An exposed cast and a fan work just as well and are safer. Cast dryers can burn skin and tend to hasten the drying time of the outer layers only.
II. BASIC PRINCIPLES OF CAST APPLICATION
A. Casts are used for the following purposes:
- To immobilize fractures, dislocations, injured ligaments, and joints; to provide relief from pain caused by infections and inflammatory processes; and to facilitate healing
- To allow earlier ambulation by stabilizing fractures of the spine or lower extremities
- To improve function by stabilizing or positioning a joint, such as for wrist drop after a radial nerve injury, which also allows more useful hand function
- To correct deformities, as in serial casting for clubfoot (see Chapter 6 for the Ponseti technique) or joint contractures
- To prevent deformity resulting from a neuromuscular imbalance or from scoliosis
B. Principles. Although plaster of paris has been used extensively in the treatment of fractures for more than 100 years, there is no unanimity of opinion as to the best technique for application. It can be safely concluded that even the tightest of skintight casts allows some motion at the fracture site, whereas a loosely fitted, well-padded cast with proper three-point fixation can provide satisfactory immobilization. Three points of force are produced by the practitioner, who molds the cast firmly against the proximal and distal portions of the extremity (two of the points) and locates the third point directly opposite the apex of the cast, as shown in Fig. 8-1. Periosteal or other soft-tissue attachments usually are required on the convex side of the cast to provide stability. In this way, a curved cast can provide a straight alignment of the extremity within it. Charnley has stated, “If a fracture slips in a well-applied plaster, then the fracture was mechanically unsuitable for treatment by plaster, and another mechanical principle should have been chosen.” Another method for providing immobilization by plaster is based on hydraulics. Fractures of the tibia do not shorten significantly when placed in a “total contact” cast. The leg is a cylinder containing mostly fluid, and when this water column is encased in rigid plaster, the cylinder does not shorten in height because tissue fluid is not compressible.
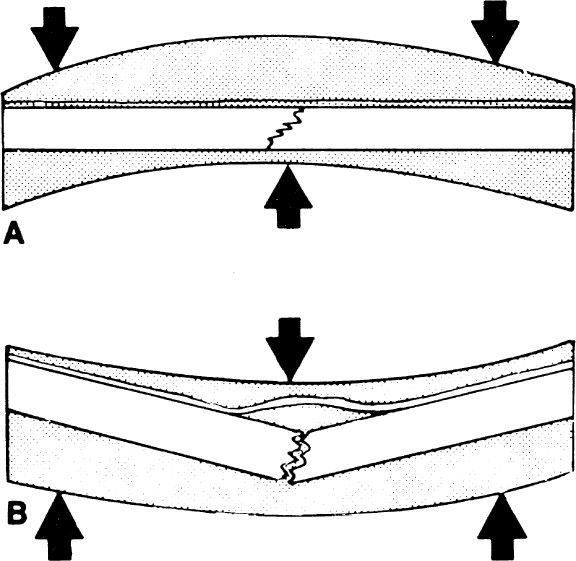
Figure 8-1. A: Three-point plaster fixation will stabilize a fracture when the soft tissue bridging the fracture acts as a hinge under tension. B: If the three forces are applied in the wrong direction, the fracture displaces.
C. The following application techniques have been satisfactory in our hands:
- The patient is informed of the procedure and instructed in whatever cooperation is necessary.
- The surgeon or cast technician must have clearly in mind what to do and what will be required (the position of the patient and assistants, how many rolls of plaster will be needed, tools to trim the cast edges, etc.). All materials and equipments required to do the job properly should be assembled. (Once cast application starts, it is difficult to stop and obtain something that was forgotten.) The patient’s position must be comfortable and must allow the surgeon and assistant to apply the cast expeditiously. Special maneuvers required to perform and hold the reduction are rehearsed.
- A circular cast should not be used in fresh trauma or postoperatively when one anticipates swelling, unless the cast is bivalved or split initially and provisions are made for adequate observation.
a. Adequate observation means an examination by a competent observer at least once hourly until any swelling begins to recede. Signs of compartmental syndrome, in order of importance, are the following: Increasing pain and discomfort in the extremity, increasing tenseness or tenderness in the involved compartment, pain with passive range of motion of the muscle in the involved compartment, decreasing sensation—especially to two-point discrimination and light touch—in the distribution of the nerves that travel through the involved compartment, increasing peripheral edema, and, finally, decreasing capillary filling. Good peripheral circulation with distal arterial pulses is no assurance that a compartment syndrome is not developing (see Chapter 3, III).
b. An excellent alternative to plaster casts in this situation is a Jones compression splint, as described in Chapter 7, III.B and C.
4. If unexpected swelling occurs in a circular cast, bivalve or split the cast immediately all the way to the patient’s skin as described in later in this chapter IV.B and C.
5. Unless specifically contraindicated, clean the part to be casted with soap and water, then dry it with alcohol. Apply the cast over a single layer of cast padding with edges of the material minimally overlapping. Protect unusual bony prominences with a ¼-in felt or foam rubber padding.
6. Dip the plaster or fiberglass rolls in water by placing them on end, and this allows air to escape and results in complete soaking of the plaster. The bandages are sufficiently soaked when the bubbling stops. They can be left in the water up to 4 minutes without decreasing the strength of the cast, but the setting time decreases with the length of time they are immersed. Therefore, for maximum working time, remove bandages soon after the bubbling stops. Lightly crimping the ends of the plaster bandages helps prevent telescoping of the roll.
7. Except for very large casts (e.g., body casts and spicas), all plaster bandages should be dipped and removed from the water at the same time. Thus, all the plaster in the cast is at the same point in the setting process. This scheme maximizes the interlocking of the crystals between the layers of plaster, thereby maximizing the strength of the cast. In addition, delamination between the bandages is decreased.
8. Use cool water for larger casts when more time is needed to apply all the plaster or fiberglass, and use warm water for smaller casts or splints. Never use hot water because enough heat can be generated to burn the patient.9 Similarly, do not place limbs with fresh casts onto plastic-covered pillows; these tend to hamper heat dispersion significantly and may result in burning. If the patient complains of burning, it is prudent to remove the cast immediately and reapply using cooler water.
9. Keep the plaster bandage on the cast padding, lifting it off only to tuck and change directions—that is, to push the plaster roll around the patient’s body or extremity. Use the largest bandages, usually 4- and 6-in bandage rolls, that are consistent with smooth, easy applications. Using large bandages allows the fastest application of plaster and provides sufficient time for molding before the critical setting period. Six or seven layers of plaster or two to three layers of fiberglass usually are sufficient, except in patients who are particularly hard on casts. The cast should be of uniform thickness (seven layers or ¼ in). Avoid concentrating the plaster about the fracture or the middle of the cast. Avoid placing two circumferential rolls directly on top of each other while wrapping the plaster on the patient’s extremity. Reinforce casts where they cross joints by incorporating plaster or fiberglass splints longitudinally. Incorporate reinforcing plaster splints into body and spica casts as described later in this chapter III.B and C).
10. During application of the cast, turn the padding back at the edges of the cast and incorporate it. Another method of finishing the edges is to turn back the padding after the cast has set and to hold the padding down with a single, narrow, plaster splint; a row of ordinary staples; or moleskin.
11. Apply all the material rapidly so there is time to work and mold it before the critical setting period. The cast should have a sculptured look, not only for cosmetic reasons but also for comfort. If the fracture is to be stabilized by the three-point fixation principle, it is more important to maintain the three forces of pressure on the cast during the critical setting period than to have a perfectly smooth surface on the cast. This step is more difficult for fiberglass casts.
12. Once the critical period of interlocking of crystals begins, molding and all motion should stop until the material becomes rigid. Otherwise, the cast is weakened considerably.
13. After the cast sets and becomes rigid, trim the edges using a plaster knife or cast saw. Use the knife by supporting the cutting hand on the cast and pulling the portion of the plaster to be trimmed up against the knife blade rather than blindly cutting through the plaster and possibly cutting the patient. If the cast is too thick or hard, an oscillating cast saw is preferred.
14. Apply forearm casts to allow full 90° flexion of all metacarpophalangeal joints and opposition of the thumb to the index and little fingers.
15. Extend leg casts to support the metatarsal heads, but not to interfere with flexion and extension of the toes. This rule is invalid when the toes need support (as with fractures of the great toe or metatarsals) or when there is a motor or sensory deficit. In these situations, the cast is extended as a platform to support and protect the toes. Place a ½-in piece of sponge rubber beneath the toes and incorporate it into the plaster for walking casts, or supply the patient with a commercial cast shoe.
16. Immobilize as few joints as possible, but as a general rule, one immobilizes the joint above and below a fresh fracture.
17. Instruct the patient regarding
a. Signs and symptoms of compression from swelling within the cast
b. Elevation of the injured part above the level of the heart for 2 to 3 days after the injury
c. How soon to walk on the cast (if appropriate and generally never sooner than 24 hours)
d. Instructions for weight bearing and ambulation; this should include crutch or walker training
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


