CHAPTER 15 Capsular Shrinkage in the Treatment of Wrist Instability
Basic Science
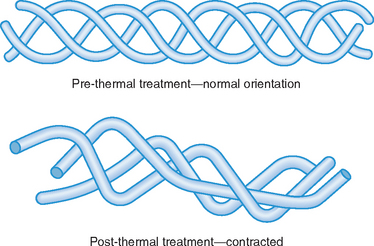
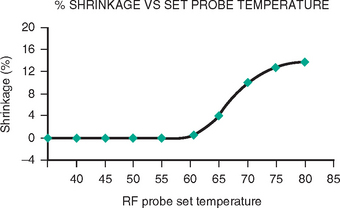
What is old is new again. Capsular shrinkage was used by Hippocrates 2,400 years ago to stabilize dislocated shoulders. Luckily, anesthetic techniques and thermal delivery methods have improved during the past two millennia. Recently (comparatively speaking), the biology of capsular shrinkage has been extensively studied in animal models. These studies have shown that the triple helix of collagen “unwinds” and “shrinks” when heated to 60° C, maximum shrinkage being achieved between 65 and 75° C (Figures 15.1 and 15.2). The hydrogen bonds that maintain the 3D configuration of the type I collagen triple–helix rupture as the collagen is heated beyond 60° C. The denatured collagen can potentially shorten to 50% of the resting length of the untreated collagen. The shortened denatured collagen acts as scaffolding onto which new collagen is deposited.1 The new collagen fibers maintain this shortened conformation, thus assuring the long–term maintenance of the shortening.
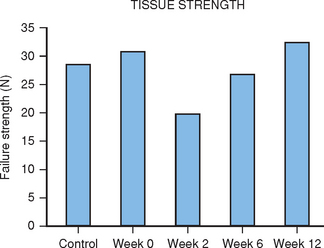
Biomechanical studies have demonstrated that the tensile strength of heated collagen decreases rapidly and does not return to normal values for 12 weeks.2 The tensile strength returns to nearly 80% normal by six weeks after heating (Figure 15.3). This transient loss of tensile strength would suggest that the application of stress to recently heated collagen is contraindicated. Premature loading of the shrunk collagen will lead to a lengthening of the collagen. This has been verified in an animal model.3,4 Based on this data, it would seem reasonable to recommend at least six to eight weeks of joint immobilization after capsular shrinkage. Clearly heavy loading of the joint should be avoided for 12 weeks.
Indications and Contraindications
Technique
Generalities
Shrinkage requires very low energy settings. The RF devices must be adjusted to heat the tissue to a temperature of between 65 and 75° C. It is wise to start at low energy and slowly increase the energy output until the desired shrinkage is observed. If a laser is used, it should be set to very low energy [i.e., 0.2 to 0.5 Joules at 15 pulses per second (3 to 7.5 Watts)]. The laser is held away from the target ligament and slowly advanced until the ligament is seen to shrink.
Once the shrinkage has stopped, continued heating will only further weaken the ligament without increasing the shrinkage. The color of the ligament changes from white to light yellow during the shrinkage. Lu et al. have suggested that a cross–hatching shrinkage pattern optimizes the in–growth of healthy tissue and hastens the recovery of the ligament.5 During the shrinkage, the traction on the wrist should be reduced as much as possible to permit optimal shrinkage.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


