Capitellum and Trochlea Fractures
David Ring
Jesse B. Jupiter
INTRODUCTION
Recent studies confirm that apparent capitellum fractures frequently involve the anterior trochlea (termed coronal shear) and often involve impaction of the posterior lateral column and the posterior and medial trochlea (1,2,3,4,5,6,7 and 8). In other words, they are often complex articular fractures of the articular surface without fracture of the columns of the distal humerus.
These fractures can be challenging to repair by virtue of (a) small entirely articular fragments, (b) limited subchondral bone, (c) small-sized fragments, (d) multiple fragments, and (e) little or no unfractured humerus to which the fracture fragments can be repaired. Involvement of the posterior humerus (posterior lateral column behind the trochlea and the posterior trochlea) has been associated with a substantial risk of nonunion (2). In our opinion, this is related to avascular necrosis with a greater risk for infection (2,3,6).
The most complex fractures may be considered for hemiarthroplasty (prosthetic replacement of the distal humeral articular surface) in older or more infirm patients with lower functional demands because the columns and the medial collateral ligament are usually intact. Total elbow arthroplasty is also an option in low-demand or infirm patients, as is nonoperative treatment or the so-called “bag of bones” technique.
PREOPERATIVE PLANNING
History and Physical Examination
Fracture of the capitellum and trochlea can occur as a fracture dislocation, so patients should be asked about any potential self-reduction or reduction by a health care provider. Complex fractures typically involve fracture of the lateral epicondyle, but fracture dislocations will also have a medial collateral ligament avulsion from the medial epicondyle (1,2).
Ulnar neuropathy is sometimes diagnosed during the recovery process, so it is worthwhile to carefully examine and document nerve function at the time of injury.
The patient’s functional demands and overall health will influence treatment as much as the fracture pattern and complexity. Circumstances such as lower limb injuries and the need for weightbearing through the upper limb for ambulation might also be important.
Imaging Studies
Computed tomography (CT) provides useful information, particularly for more complex fractures. We find 3D reconstructions more intuitive, and there is some evidence that they can improve the reliability of diagnosis of certain fracture characteristics (9) (Fig. 9-1). It is helpful to be prepared for the size and extent of the trochlea fracture (involvement of the posterior or medial trochlea in particular) and any fracture of impaction of the posterior aspect of the lateral column (Fig. 9-1B and C). The extent of fragmentation can also help with planning of either fixation techniques or the decision to use a prosthesis. One thing to look for carefully is stable impacted fracture fragments (Fig. 9-1B). These fragments are out of position but may not appear fractured in surgery because they are not easily moved and the fracture lines are not obvious (analogous to plastic deformation in children). It may not be possible to fully reduce all the fracture fragments until these fragments are realigned.
 FIGURE 9-1 Three-dimensional computed tomography (3DCT) reconstructions with the radius and ulna subtracted can be very helpful for defining the extent of the injury and planning surgery. A: This 3DCT image shows that the entire capitellum and the anterior part of the trochlea are a single large fracture fragment. The lateral epicondyle is fractured, which can facilitate exposure. There is little or no fracture or impaction of the posterior structures, which will make this a relatively straightforward fracture to expose and repair. B: In this 3DCT image, there is a large capitellum/trochlea fracture and a lateral epicondyle fracture, but there is also fracture of the posterior part of the lateral column, and the medial part of the trochlea is fractured and impacted/rotated upward. The posterior trochlea may also be fractured, and other views confirmed that it was. This is a complex fracture that should be treated through an olecranon osteotomy. C: This 3DCT shows that the entire articular surface is fractured into several fragments. |
Timing of Surgery
It is more important that a surgeon who is familiar with these fractures treats the patient with adequate preparation (e.g., CT scan) and appropriate equipment available than it is to do the surgery soon after injury. A delay of up to 2 weeks to get all of this organized is reasonable. The exception is the rare open fracture. It is difficult to stage the treatment of open fractures because some of the important articular fragments are completely devitalized and benefit debridement, irrigation, and repair at the time of open fracture treatment to limit colonization and the potential for infection.
SURGERY
Positioning/Surgical Approaches
The majority of capitellum/trochlea fractures can be treated through an extended lateral exposure, which is easiest with the patient supine and arm supported on a hand table (Figs. 9-2, 9-3 and 9-4). When
there is involvement of the posterior or medial part of the trochlea, an olecranon osteotomy provides better access and visualization (Fig. 9-5).
there is involvement of the posterior or medial part of the trochlea, an olecranon osteotomy provides better access and visualization (Fig. 9-5).
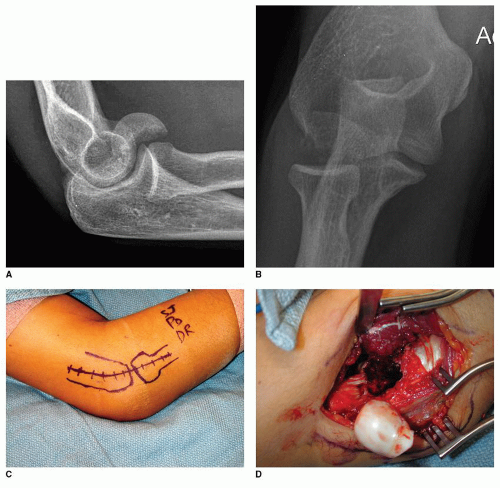 FIGURE 9-2 A 30-year-old woman fell and fractured her distal humerus. A: A lateral radiograph shows a capitellum fracture. B: The anteroposterior radiograph suggests that the fracture is relatively simple. C: A lateral skin incision is planned. This can be either straight or curved. D: The radial wrist extensors are elevated off of the supracondylar ridge, and the interval between the extensor carpi radialis brevis and the extensor digitorum communis is developed distally, staying anterior to the midpoint of the radial head to preserve the lateral collateral ligament. The fracture fragment involves the anterior part of the lateral trochlea and has very little soft tissue attachment. |
For simple fractures, a lateral skin incision is sufficient (Fig. 9-2C). For more complex fractures, a posterior skin incision allows the surgeon to convert to an olecranon osteotomy when necessary (Fig. 9-3A




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
