Sterile Instruments/Equipment
- Tourniquet
- Headlight
- Large pointed bone reduction clamps (Weber clamps)
- Laminar spreader
- Dental picks and Freer elevators
- Shoulder hook
- Schanz pins (2.5 to 4.0 mm)
- Femoral distractor (small)
- Implants
- Mini- and small-fragment screws and mini-fragment plates (2.0/2.4/2.7/3.5 mm)
- Calcaneal plates, locking or nonlocking
- Autograft, cancellous allograft, or other bone substitute for structural defects
- Mini- and small-fragment screws and mini-fragment plates (2.0/2.4/2.7/3.5 mm)
- K-wires and wire driver/drill
Positioning
- The patient is positioned in the lateral decubitus position.
- Take care to pad all bony prominences, including down greater trochanter, fibular head (peroneal nerve), and elbow (radial nerve).
- See the chapter (1) for full description.
Surgical Approach
- Extensile lateral approach, as described by Benirschke and Sangeorzan.1
- Vertical limb should be approximately 1 cm anterior to the Achilles tendon.
- The vessel that supplies the flap can be located with a Doppler.
- Proximal extension of the vertical limb should be performed without injuring this vessel.
- Take caution not to injure the lateral calcaneal artery, which is directly across the vertical limb and supplies the majority of the flap (Fig. 26-1).
- The vessel that supplies the flap can be located with a Doppler.
Figure 26-1. Doppler showing the position of the arterial inflow to the lateral heel flap.
![]()
- To determine the course of the sural nerve, mark a point one thumb breadth posterior to the distal tip of the fibula, and connect it to the base of the fifth metatarsal (Fig. 26-2).

Figure 26-2. The approximate course of the sural nerve based on the fibula and the fifth metatarsal.
![]()
- Gently curve incision, make horizontal limb along the glabrous border of the heel (Fig. 26-3).
Figure 26-3. The lateral extensile incision.
- Meticulous subperiosteal elevation of soft tissues off of the lateral wall.
- Place small rakes under periosteum, and avoid separating soft tissue layers.
- Elevate the calcaneofibular ligament.
- Dissect beneath the osseous reflection of the peroneal sheath, and elevate the peroneal tendons anterosuperiorly.
- 0.062 inch K-wires can be inserted into the fibula and talus, and bent for soft tissue retraction.
- Be mindful of point pressure on soft tissues.
Reduction and Fixation Techniques
- Spanning calcaneus external fixation (Figs. 26-4 and 26-5).
- Place the frame medially to preserve lateral soft tissues for lateral exposure after soft tissues heal.
- A medial incision is made over the medial cuneiform.
- A 170 mm × 5.0 mm Schanz half pin is placed from the medial to the middle of the lateral cuneiform.
- A second 170 mm × 5.0 mm Schanz half pin is placed via the percutaneous incision through the medial tibia to provide a point of fixation on the tibia.
- External fixation clamps are then applied and a bar is placed from the cuneiform pin to the tibial pin.
- A third 5.0 mm Schanz pin is placed in the calcaneal tuberosity via a medial incision, and a distraction is then applied via a pin-bar clamp to the already established bar apparatus from the medial cuneiform to the tibia, forming a “T.”
- A distraction vector of height, length, and translation is facilitated to disimpact the fracture.
- This facilitates the restoration of anatomic height and length at the time of definitive reconstruction.
- Additional distraction vectors can be applied as needed through additional bars.
- A laminar spreader between two pin-bar clamps or a pin-bar clamp and a universal chuck can be used to medialize the tuberosity fragment.
- After the distraction has been achieved, lateral, axial, and AP views of the foot document the position of the pins and distraction that is achieved.
- Place the frame medially to preserve lateral soft tissues for lateral exposure after soft tissues heal.
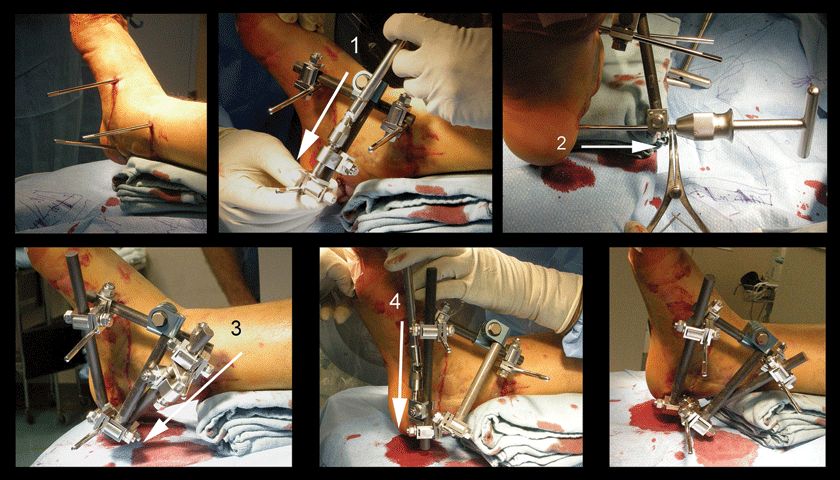
Figure 26-4. Calcaneal external fixation placement. Half pins are placed medially in the cuneiforms, the calcaneal tuberosity, and the distal tibia. Length is reestablished initially (1), followed by reduction of the tuberosity varus and translation (2). Height and length are once again fine tuned (3, 4).

Figure 26-5. After placement of Schanz pins in the distal tibia, cuneiforms, and calcaneal tuberosity (top row), the calcaneal height, length, varus, and translation are progressively reduced (second and third rows).
Tongue-type Fractures
- High vigilance must be maintained for threatened posterior soft tissues.2
- Tongue variant with impaction
- Via a small incision posteriorly, a Schanz pin is placed into the tuberosity to provide a manipulative reduction of the tuberosity and to disimpact the articular segment from the critical angle of Gissane (Fig. 26-6).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


