14 Bowel obstruction



Mechanical obstruction
Figure 3.14.1 shows areas of potential mechanical obstruction. Sigmoid volvulus appears as an ‘inverted U’ or ‘rugby ball’ on abdominal radiograph; if a flatus tube cannot decompress the obstruction, surgery is indicated. In a closed loop obstruction (Fig. 3.14.1D), the large bowel contents distend the thin-walled caecum because a competent ileocaecal valve prevents reflux. The risk of perforation is very high. Right iliac fossa tenderness becomes constant or localized if perforation is imminent. An incompetent valve allows reflux (20% of cases), causing vomiting. Strangulation occurs in unresolved bowel obstruction; occlusion of venous return will later block arterial supply to the affected loop, leading to infarction and perforation, and subsequent peritonitis. It is commonly caused by an obstructed hernia (check the hernial orifices) or volvulus. Signs of strangulation are rapid worsening in general condition, sharp and constant pain, increasing fever and heart rate, worsening peritonitis and a raised white cell count.
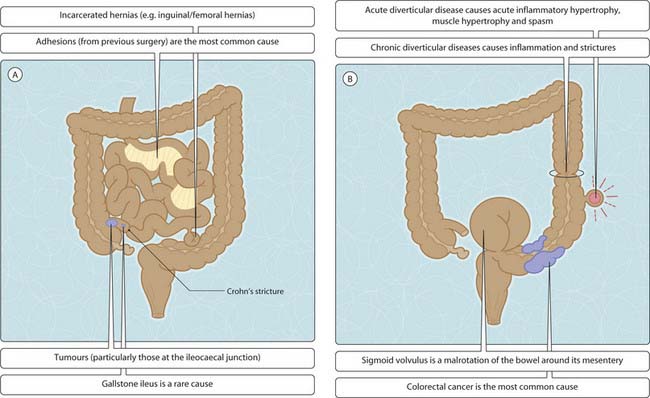
Fig. 3.14.1 Bowel obstruction. (A,C) small; (B,D) large. Table 3.14.1 lists the features that can be identified in (C) and (D).
< div class='tao-gold-member'>




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


