Fig. 23.1
Lower anchor bars embedded in vehicle seat
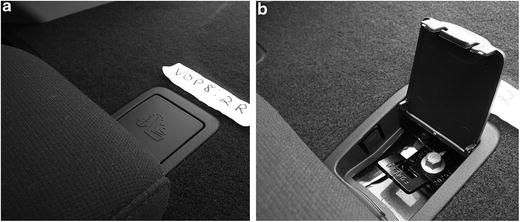
Fig. 23.2
Tether anchor hardware
For US child restraints, most products attach to the lower anchors using a length of webbing with connectors and adjustment hardware on each end. CRS lower connectors are usually hook-on or push-on styles (Fig. 23.3). Many products route the LATCH strap through the vehicle belt path on the child restraint rather than using a seatbelt (Fig. 23.4a), or attach them to each side of the child restraint (Fig. 23.4b). A few US products use rigid lower LATCH connectors (Fig. 23.4c), which are required by ISOFix in Europe. Although products must meet FMVSS 213 excursion requirements when tested without a tether, the tether improves occupant protection in forward-facing restraints by reducing child head excursion when used with either the vehicle seat belt or the LATCH strap. Also, the tether often helps to obtain a better installation.
Fig. 23.3
Hook-on (top) and push-on (bottom) LATCH strap connectors
Fig. 23.4
Implementations of LATCH on US child restraints: LATCH strap routed through belt path (top), attached to bar on each side (center), rigid LATCH (bottom)
LATCH does make child restraint installation easier in some vehicles compared to using the seatbelt. But in others, the characteristics of the LATCH hardware can make them difficult to use [54, 55]. Instead of reducing misuse, LATCH often results in new types of misuse. Notably, only about half of caregivers use the top tether with forward-facing products [15, 56]. In a study of vehicle LATCH hardware characteristics, lower anchors more than 2 cm within the vehicle seat bight, high attachment forces, and low clearance around the lower anchors increase the likelihood of installation errors [57].
Another issue with LATCH relates to the strength of the anchorages. FMVSS 225 specifies a quasi-static pull test to evaluate the lower and tether anchorages. Since most harnessed child restraints were designed for children weighing up to 18 kg (40 lb) when LATCH was first introduced, some vehicle manufacturers have stated that LATCH hardware could only be used for children up to this weight. However, child restraints have become heavier as they incorporate more ease-of-use and side impact protection features. They have also been designed to accommodate larger children using a harness, with some products allowing harness use up to 39 kg (85 lb). NHTSA issued regulation changes indicating that anchors designed to meet the quasi-static strength requirements should be strong enough to secure a combined weight of 29 kg (65 lb) for the child and child restraint [58]; child restraint manufacturers must label the acceptable child weight range based on the weight of the product. With some child restraint weights exceeding 11 kg (25 lb), this limits the ability to use lower anchors to secure the product over its usable lifetime. All child restraints can still be installed with the seatbelt as the primary connection, but there are concerns that caregivers will not realize the need to transition from LATCH to seatbelt securement and failures may occur.
In some cases, seatbelts may provide a better install than LATCH for any weight of child because of incompatibilities. Best practice recommends that a child restraint should be installed using the method that most easily provides a tight installation. All forward-facing installations should use a tether. In their statement regarding limits for lower anchors, NHTSA did not specify limits for tether anchors. Since the top tether supplements the main securement method, and provides a safety benefit by reducing head excursion, they should be used consistently despite a small risk of injury from a hypothetical tether anchorage failure in a severe crash.
23.3.3 Usability and Vehicle/Child Restraint Compatibility
Although vehicle LATCH hardware designs and child restraints have often improved, incompatibility between some vehicles and some child restraints continue to cause installation issues. Misuse of child restraints continues to be a problem. Several different approaches have been implemented to make child restraints easier to use; FMVSS 213 only deals with usability peripherally relative to requirements for labeling and manuals.
A consumer information program, the Ease-of-Use (EOU) Rating system [59], has been developed by NHTSA to publish information about different features available on child restraints. The rating system has promoted positive changes in child restraint products, leading to development of innovative features. To address vehicle/child restraint compatibility, NHTSA has proposed an additional consumer information program where vehicle manufacturers would list child restraints that “fit” in particular vehicles based on a specific set of key installation factors [60].
The Child Restraints Group of the ISO has developed a three-part evaluation system that assesses the usability of ISOFIX (LATCH-type) hardware. The system addresses child restraints, the vehicle environment, and the interaction between specific pairings of child restraints and vehicles [61, 62]. Several of the vehicle features assessed include elements of the vehicle owner’s manual, labeling and visibility of anchors, the ability to confuse the anchors with other vehicle hardware, the actions required to prepare the anchors, and incompatibilities between anchors and seatbelts.
A recommended practice has been drafted by the SAE Children’s Restraint Systems Standards Committee with the goal of improving compatibility when child restraints are installed in vehicles using LATCH [63]. The document describes procedures and tools to assess vehicle and child restraint hardware. Vehicle factors include measuring the clearance around lower anchorages, and measuring the force required to attach lower connectors, while child restraint factors include maximum and maximum sizes for the dimensions of LATCH connector hardware.
23.4 Child Restraint Systems
Best practice recommendations for proper child restraint include four main stages: rear-facing harnessed restraint, forward-facing harnessed restraint, booster seat with a lap-and-shoulder belt restraint, and seat belts. Both the child’s maturity level and physical size influence the proper choice of restraint for a child. Because each step in the sequence reduces the level of occupant protection, children should delay moving to the next level as long as possible.
23.4.1 Rear-facing Child Restraints
Since 2011, both the National Highway Traffic Safety Administration and the American Academy of Pediatrics recommend that children travel rear-facing until they no longer fit in their restraint. Based on available products and typical child sizes, most children in the US should be able to travel rear-facing through the age of 2 years. Henary et al. [8] analyzed NASS-CDS data and found that children aged 0–2 years in rear-facing restraints are 5.53 times safer in side impacts than children in forward-facing restraints; the comparable ratio is 1.23 in frontal impacts. These limited US data agree with results from Sweden (where best practice keeps children rear-facing through age 4 years) showing that the risk of AIS2+ injury is 90 % lower for rear-facing children than unrestrained children [64, 65]. Older educational materials may include text stating that children only should remain rear-facing through age 1 or 10 kg (20 lb), but this is no longer considered a safe practice.
Two styles of rear-facing child restraints are currently sold in the US. Infant or rear-facing only restraints typically have a shell portion (with carrying handle) to secure the child that are attached to the vehicle using a separate base to simplify repeated installation (Fig. 23.5a). However, most can be secured with the seatbelt without the base (Fig. 23.5b). Either the seatbelt or lower anchorages can be used to attach to the vehicle. These products are designed to restrain children between 9 and 16 kg (20–35 lb). Rear-facing convertible products (Fig. 23.5c) can be used rear-facing for children weighing up to 13–20 kg (30–45 lb), and are then converted to use in forward-facing mode. Best practice for rear-facing use dictates that the top of the child’s head should have at least 2.5 cm (1 in.) clearance to the top edge of the child restraint. Many children will outgrow their rear-facing restraint by length before they reach the maximum weight.
Fig. 23.5
Rear-facing child restraints: rear-facing only with base (left), rear-facing only without base (middle), and convertible installed rear-facing (right)
The internal harness of a rear-facing restraint secures the child within the shell. However, the main restraining forces in a frontal impact are provided by the back of the child restraint and distributed across the head and back of the child. The head and neck are supported in the same way as the torso, which reduces the tension and flexion forces that can occur on the neck with forward-facing children. Figure 23.6 shows a sequence illustrating the difference in head kinematics during a simulated frontal impact when the same child restraint is used rear-facing and forward-facing. The peak axial neck forces with the forward-facing restraint are four times higher than the dummy restrained in the rear-facing restraint.
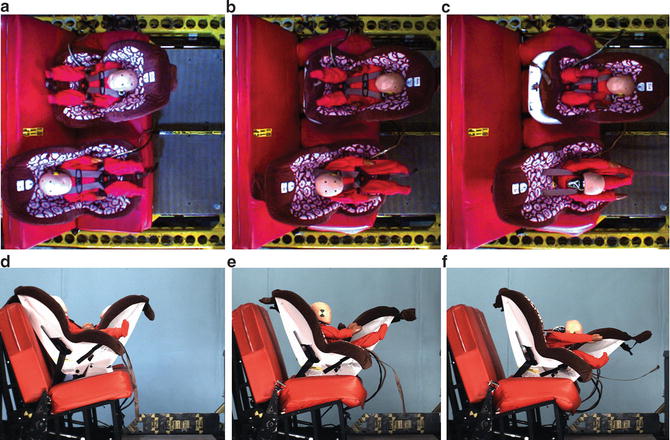
Fig. 23.6
Sequence showing advantage of using rear-facing child restraint compared to forward-facing child restraint
Misuse of rear-facing restraints include forward-facing use, which could result in injurious loading or ejection because the belt path was not designed for this loading direction. If a convertible restraint is installed rear-facing using the forward-facing belt path (or vice versa), similar negative consequences could occur. Allowing a child to travel forward-facing too early increases spinal cord injury risk; the youngest children’s heads comprise a larger proportion of their body mass, resulting in greater tensile load to the cervical spine to stop forward head motion.
When installing rear-facing child restraints, achieving the correct angle is critical. A rear-facing restraint installed too upright may cause the small infant’s head to tip forward and impair breathing. A rear-facing restraint installed too reclined will not allow the back of the restraint to effectively restrain the child.
In a frontal crash, the ability of the restraint to restrain the child decreases as the angle of the back support is reclined more than 45°, because the force projecting the baby upwards along the seatback becomes larger than the reaction force provided by the back of the child restraint. For larger rear-facing children, placing the restraint more upright would allow better crash protection. For newborns, the child restraint angle must balance between crash protection and keeping the head from hanging forward and potentially cutting off the airway. A back support angle of 45° (shown in Fig. 23.7) from vertical is considered the best compromise between these two opposing issues.
Fig. 23.7
Angles for rear-facing child restraints
Because installation angle varies with the geometry of the vehicle seat, child restraint manufacturers usually provide some sort of angle indicator to provide guidance during installation. However, indicator placement is often based on where the child restraint performs best in FMVSS 213 testing. Some child restraint products now have different angle indicators for smaller and larger children that account for the changing needs of rear-facing children, but not all manufacturers do so. For newborn children, if the required installation angle based on manufacturer instructions places the child too upright, parents should switch to another rear-facing child restraint or car bed.
When rear-facing child restraints are installed in the rear vehicle seat, allowing the back of the restraint to initially contact the back of the front seat will limit forward rotation and improve protection during a crash. Forces can be higher if there is an initial gap and the child restraint then suddenly contacts the seatback [66, 67]. This initial configuration is not allowed by some vehicle manufacturers because the contact can interfere with the occupant sensing systems used with advanced airbags. Some child restraint manufacturers also prohibit the initial contact because of concerns regarding potential adverse interaction in rear impacts between the child restraint and front seatback.
Some child restraint manufacturers recommend using a tether with rear-facing child restraints. This practice is not covered by FMVSS 213, which specifies that child restraints meet requirements without using a tether. FMVSS 225 also does not specify tether anchors located below and forward of a vehicle seating position that can be used with a rear-facing child restraint. Tethering rear-facing child restraints is more common in Scandinavia and Australia. The Australian method (Fig. 23.8a) routes the tether towards the back of the vehicle and uses the same tether anchorage used with forward-facing child restraints. This tethering strategy prevents forward movement and rotation. The Swedish method (Fig. 23.8b) routes the tether to a point forward and below the vehicle seat to help control the initial restraint angle and limit rebound rotation towards the back of the vehicle [68].
Fig. 23.8
Tethering rear-facing child restraints: Australian method (left) and Swedish method (right)
When evaluating the effect of tethering rear-facing during laboratory testing, any type of rear-facing restraint, with or without tether, provided better protection than a forward-facing restraint with a tether. Among the rear-facing conditions, the Australian tether method led to the lowest head and chest accelerations, as well as the lowest forward head excursions. During simulated rear-impact testing, none of the tethered rear-facing conditions produced excessive neck loads relative to the injury reference values listed in FMVSS 208 [69].
As in other crash modes, the first priority of a restraint system during side impact is to prevent head contact. If preventing head contact is not possible, the object that the head contacts should be designed to absorb energy. Because of the differences in belt path locations and the child’s center of gravity between rear-facing and forward-facing child restraints, a rear-facing restraint will move more towards the side of impact relative to a forward-facing child restraint. Despite this greater motion, analysis of crash data indicates that children in forward-facing child restraints are five times more likely to sustain serious injury in side impacts compared to children in rear-facing restraints [8]. Because most side impacts have a frontal deceleration component, occupants will move toward the struck side and towards the front of the vehicle. This frontal deceleration component will cause the head of a rear-facing child to move further into the shell within the side wings of the restraint, while the head of a forward-facing child moves forward out of the protective sides of the restraint, exposing it to potential contact from intruding vehicle components. Child restraint systems equipped with rigid LATCH connectors reduce movement of both the child restraint and child in side impacts, improving the ability to prevent head contact [70].
Rear-facing child restraints can rotate towards the rear vehicle seatback during rear impacts and rollovers. In these situations, the harness provides the main occupant restraint. When rear-facing child restraints were first introduced, the designers envisioned this “cocooning” movement as a benefit to shield infants from debris [71]. With the development of larger rear-facing restraints designed to accommodate larger children, there is greater potential for head contact with interior vehicle components during a rear impact or rollover. However, no crash investigations have documented head injuries from this injury mechanism to date.
Most rear-facing child restraints employ a five-point harness, although previous designs used a three-point harness that did not have straps routed over the hips. To provide child restraints that can accommodate children weighing from 2 up to 18 kg (4 to up to 40 lb) rear-facing, child restraint manufacturers have provided more adjustable harnesses, a greater number of shoulder slots, and padded inserts. Padding should not be used if it pushes the infant’s head toward the chest. If needed for lateral support, additional firm padding such as a rolled blanket or towel can be placed between the infant and the side of the restraint. To prevent slouching, caregivers can place rolled towels between the infant and crotch strap [72]. However, thick soft padding should never be placed between the back of the restraint and the child or between the child and the shoulder straps. Unless tested and provided by the child restraint manufacturer, this type of padding would create harness slack as it compresses during dynamic loading, potentially leading to ejection of the child or excessive loading during a crash.
To fit the harness to a rear-facing child, use the shell harness slots that are at or below the child’s shoulder height. If higher harness slots are used, the child could slide up the seatback during a crash, possibly allowing the child’s head to move beyond the protective shell of the child restraint. With smaller babies, the head would likely be retained within the shell if higher slots are incorrectly used, but using higher slots could increase loading through the shoulders. Loose harnesses increase the level of loading and the likelihood of ejection. During a crash, chest clips help keep the harness positioned on the shoulders but cannot compensate for a loose harness.
Despite advances in frontal impact airbag systems, the right-front passenger seating position should never be used for rear-facing child restraint installation. A rear-facing child restraint installed in the right-front passenger seating position places the child at high risk of injury or death during a crash. For a rear-facing child installed in the right-front position, the child’s head is placed very close to the airbag module. To provide an adult occupant with energy-absorbing cushion of restraint during a crash, the airbag must deploy at high speed from a small folded package, as much as 300 km/h (186 mi/h). The force of an airbag contacting the back of a rear-facing child restraint during inflation produces accelerations in infant dummy heads from 100 to 200 g [73, 74], with 50 g considered the injury threshold for children the size of a 6-month-old dummy [74, 75]. Figure 23.9 shows an airbag contacting a rear-facing child restraint. Laboratory measurements indicate that head injuries occur from the initial contact, even though the airbag can also rotate the infant and restraint into the vehicle seatback.
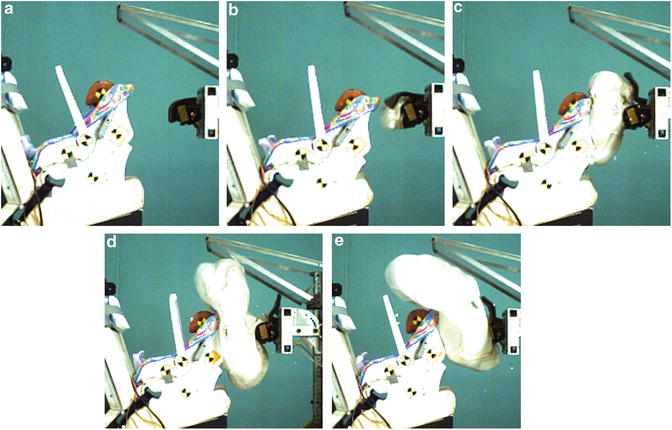
Fig. 23.9
Airbag deployment into a rear-facing child restraint
23.4.2 Car Bed Restraints
A car bed (Fig. 23.10) is a suitable choice for infants with medical issues that prevent them from using the semi-reclined position provided by a rear-facing restraint system. Car-bed restraints allow the infant to lie flat, usually on its back. A car bed is installed with its length perpendicular to the fore-aft direction in the vehicle, with the baby’s head placed nearest the vehicle center.
Fig. 23.10
Example of a car-bed restraint
During frontal crashes, the side of the car bed restraint distributes restraining forces along the length of the infant’s body. During rebound or rollover, the harness provides the restraint. Although there are no documented field data, infants in car beds during side impacts may be more likely to sustain head or neck injury than those in rear-facing restraints, particularly if the head is closest to the struck side of the vehicle [76].
Rear-facing restraints are the first choice of the American Academy of Pediatrics for infants, but they acknowledge that positional apnea may require use of a car bed [77–79]. Current best practice for infants born at less than 37 weeks gestation is to evaluate them before hospital discharge to detect possible apnea, bradycardia, or oxygen desaturation that might occur during use of a rear-facing child restraint [80].
23.4.3 Forward-Facing Child Restraints
Children traveling forward-facing in a harnessed restraint system can either use a convertible child restraint in the forward-facing mode (Fig. 23.11a) or a combination child restraint equipped with a harness that can be reconfigured into booster mode (Fig. 23.11b). Some products are available that are designed for only forward-facing harnessed use.
Fig. 23.11
Forward-facing convertible (left) and combination restraint used in forward-facing harnessed mode (right)
While the maximum child weight limit of some forward-facing restraints is up to 22 kg (40 lb), many child restraints allow children up to 40 kg (90 lb) to use the harness system. All forward-facing child restraints sold in the US can be installed with either a seatbelt or LATCH lower attachments. In addition, all child restraint manufacturers currently recommend that the tether be used with forward-facing child restraints to minimize forward head movement during a crash.
The best protection of a forward-facing child requires a snug fit of the harness and tight installation of the child restraint to couple it to the vehicle. Most current child restraints use a five-point harness (Fig. 23.12a) because they permit the best snug fit around the child. However, a few child restraint models use a tray shield, shoulder straps, and crotch strap (Fig. 23.12b) to secure the child.
Fig. 23.12
Forward-facing restraints with 5-point harness (a–left) and tray shield (b–right)
The five-point strap harness design is based on restraint systems used by race car drivers and the military. The five “points” are a strap over each shoulder, a strap over each hip, and a crotch strap between the legs. Many products use a harness adjuster that tightens the harness with a single pull or twist of a knob. If the harness is loose rather than snug, the child can move closer to vehicle components at the onset of the impact and experience higher acceleration levels when they eventually load the harness. Ejection or injury to the thorax or abdomen can occur with a misrouted or improperly buckled harness.
With forward-facing restraints, the shoulder straps should be placed through harness slots that are at or above the child shoulders. If the harness is routed to slots below the shoulders, it essentially introduces slack to the system, since the child can move forward before the harnesses start to restrain the shoulders. Sometimes the lower slots on convertible restraints are not strengthened for use in forward-facing mode; using these slots for forward-facing could lead to failure of the child restraint shell.
Switching a child from rearward-facing to forward-facing should be delayed as long as possible, because rear-facing is the safest mode of child restraint. When forward-facing in frontal crashes, the cervical spine experiences significant loading as the harness holds back the shoulders and the head moves forward and is stopped by the neck. In a frontal 48 km/h (30 mph crash) with a vehicle compartment deceleration of 25 g, the occupant’s head stops later and more abruptly than the vehicle and can experience deceleration levels of up to 60 or 70 g. The strength of the vertebrae and connecting ligaments determines whether the spinal cord will be injured [81, 82]. In adults, the cervical spine is fully ossified and can experience tensile forces corresponding to decelerations of up to 100 g [83], so spinal cord injury is almost always accompanied by vertebral fracture. With children, the flexible characteristics of the cervical spine that allow growth permits children to sustain injury to the spinal cord even if the vertebrae remain intact [84–86]. Spinal cord injury risk decreases with age and increases with crash severity [82]. Although serious cervical spine injuries are rare among forward-facing children using proper restraint, crash investigations provide evidence of serious long-term negative consequences from spinal cord injury [73, 87–90]. Because of the potential for negative consequences from cervical spine injuries, best practice recommends keeping smaller children rear-facing as long as possible.
To reduce forward rotation of the child in frontal crashes, caregivers should always use top tethers with forward-facing child restraints [91, 92]. The kinematics of a forward-facing harnessed 3-year-old dummy restrained with a tether (closer to camera) and untethered (farther from camera) in a frontal 48 km/h crash are shown in Fig. 23.13. With a tethered child restraint, head excursion is an average of 150 mm (6 in.) less than the untethered child restraint. Less head excursion during a crash translates to lower likelihood of interior head contact. Head and face injuries are most common among children injured in forward-facing child restraints [93–95]. Although rare, head contact can also lead to vertebral fractures and dislocations, as well as spinal cord injury [82, 83], so reducing head excursion and contact can also reduce risk of neck injury. Using the top tether can also improve coupling between the vehicle and child restraint. But the tether must be tight, as slack degrades tether effectiveness. About half of caregivers fail to use tethers with forward-facing installations, making it a leading type of misuse [56].
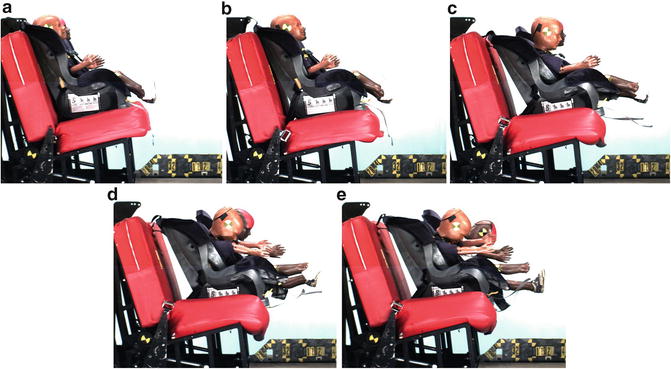
Fig. 23.13
Sequence of photos showing reduced excursion when tether is used (nearest to camera)
While frontal impacts occur more frequently, risk of serious or fatal injury is higher in side impacts [96]. The transition from rear- to forward-facing restraints should be delayed because the risk of injury in side impacts is so much lower for rear-facing children [8]. Forward-facing restraints with larger padded sidewings may offer improved protection when attempting to prevent injuries to the most commonly injured regions of the head and face [97–99]. In addition, child restraints with rigid LATCH connectors were better at preventing rotation towards the struck side of the vehicle during laboratory testing [70]. However, the same series of tests showed negligible benefit of the tether on lateral head excursion during side impact. Some child restraints now include additional energy absorbing elements, such as a side air cushion, which show potential for improved side impact protection [100].
Like all children under age 13, those in forward-facing child restraints should use a rear seating position. However, if the rear seat is fully occupied with other children, a properly restrained child in a forward-facing harnessed restraint would be the best choice for the right-front seat. Risk of injury from the airbag for such a child should be similar to the risk of a belted adult. Compared to a child in a booster seat or seatbelt, the harness prevents the child from leaning forward and being too close to the airbag. None of the children who sustained fatal injuries from deploying airbags were properly using a forward-facing child restraint [37]. If a child in a forward-facing restraint is using the right-front seating position, the vehicle seat should be placed as rearward as possible while allowing use of the rear seat.
23.4.4 Boosters
Children who can no longer fit in a harnessed forward-facing restraint should switch to a belt-positioning booster seat used with a vehicle lap-and-shoulder belt. Because the risk of injury is lower for forward-facing children in harnessed restraints compared to children using boosters, the transition should be delayed as long as possible. Booster seats reposition the child and redirect vehicle belts to improve their routing relative to the child’s body, but do not actually restrain the child. According to both the NHTSA and the AAP, children should use booster seats until they fit in seat belts alone. This means most children should use boosters through age 8–12 years [2]. As a result of public education programs, state laws requiring boosters, and more available booster products, use of booster seats among children aged 4–8 years has risen from 15 % in 2000 to 63 % in 2007 [13].
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


