Chapter 24 Behavioral Problems in Children and Adolescents
Behavioral problems are common reasons for parents to bring their child to see the family physician. In addition, addressing behavioral issues is an important component of the well-child visit. Childhood behavioral problems are a complex assortment of individual mental disorders, genetic and medical disorders, family interaction difficulties, social and school problems, and combinations of these. The rates of many psychosocial problems in children and adolescents, including depression, suicide, conduct disorders, and drug and alcohol abuse, have been rising in recent years throughout Western culture (Fombonne, 1998). This increase is only partly explained by changes in diagnostic criteria and reporting. The trend is particularly troubling when economic conditions and physical health of the population have been improving. The implication for office physicians is that psychosocial problems will encompass a growing proportion of patient care both as presenting problems and as cofactors in other medical conditions.
This chapter is arranged in problem-focused fashion along a developmental continuum from infancy through adolescence based on when various problems are most frequently encountered in practice. For conditions encountered at different developmental stages, discussions include similarities and differences in recognition and treatment at different ages. Management focuses on early, brief interventions the physician can make with the patient and family as well as suggestions about referral.
Regardless of the behavioral concern or the child’s age, general principles for evaluation and management include the following:
For adolescents with more serious emotional or behavioral concerns, outpatient care may not always provide enough structure on its own. Some teens may need a higher level of support that includes therapy, daily routines, family involvement, medication management when appropriate, and guidance from trained mental health professionals. In these cases, Avery’s House residential mental health treatment center for teens in Boise can be a relevant example of a structured care option for teens, while families in other areas, such as Phoenix, may also look for similar residential programs when brief interventions or weekly appointments are not enough. A residential setting can help teens work on emotional regulation, behavior patterns, coping skills, and healthier daily habits in a more supervised therapeutic environment.
Sleep Problems
Normal sleep has a well-characterized pattern of rapid eye movement (REM) and non-REM sleep that changes with age. Non-REM sleep is further categorized into stages 1, 2, 3, and 4, on the basis of electroencephalographic (EEG) characteristics, with the deepest non-REM sleep occurring in stages 3 and 4. A normal nighttime sleep cycle is about every 90 minutes, with multiple brief arousals and quick returns to sleep without memory of having awakened. Deep non-REM sleep predominates in the first several hours of sleep, and REM is most prominent in the last few hours. Children have substantial periods of very deep sleep that lessen with age. There is a gradual decrease in the amount of REM sleep and a significant decrease in deep non-REM sleep, especially in adolescence.
Children and adolescents in American society sleep less than those in other societies and less than children in the past (Dahl, 1998). Because of the wide variations in normal sleep patterns and development, the physician should avoid rigid expectations in counseling parents, but the following are some useful guidelines. A typical infant is able to sleep 6 to 8 hours through the night by age 2 months and 10 to 12 hours by age 6 months. The child usually no longer requires a morning nap by about 1 year of age and outgrows the afternoon nap around age 3. The total daily sleep requirement decreases with age, from 16 1⁄2 hours at 1 week of age to 14 hours by age 1 year, 13 hours by age 2 years, 12 hours by age 3 years, 11 hours by age 5, and 10 hours by age 9 years (Blum and Carey, 1996).
An important aspect of preventing sleep problems is guidance regarding good sleep hygiene (Box 24-1). Sleep hygiene refers to the conditions that are most conducive to healthy, restorative sleep. Some children are reassured by a low-wattage night-light, but more light than that may disturb sleep. Parents of newborns should be counseled to put their infant to sleep supine rather than prone, unless there is a specific medical indication to the contrary. This results from the association of the prone sleeping position with sudden infant death syndrome (SIDS) in young infants (Guntheroth and Spiers, 1992) (SOR: A). Many children rest better with a “transitional object,” a favorite blanket or toy. However, parents should avoid putting the child to bed with a bottle left in the mouth because it may lead to severe dental caries. Finally, the child should be put to bed awake, so that the child develops self-soothing skills to initiate sleep and resume sleep after nighttime disruptions.
About 20% to 30% of children and adolescents have sleep problems that are a serious concern to them and their families (Dahl, 1998). Problems with sleep initiation and nighttime awakenings are most common during infancy. Parasomnias and obstructive sleep apnea syndrome are most common in the 3- to 8-year-old group. Sleep deprivation, delayed sleep-phase syndrome, and narcolepsy are important considerations in the adolescent age group (Carskadon and Roth, 2000).
Besides sleep problems being common, family physicians need to be alert to these conditions because they have such a negative impact on many aspects of physical, mental, and social well-being. Sleep problems early in life are predictive of many later behavioral and emotional problems (Dahl, 1998). Children with frequent nighttime awakenings are at increased risk for physical abuse, perhaps because parents of these children show increased levels of fatigue, irritability, and depression.
The assessment and management of sleep problems in general should include consideration of potential sleep interrupters as primary causes or as exacerbators. One important category of interrupters is conditions that cause pain or itching (e.g., juvenile rheumatoid arthritis, migraine, atopic dermatitis). Another category is problems that lead to respiratory symptoms, including nocturnal asthma, gastroesophageal reflux (GERD), and obstructive sleep apnea.
Sleep Refusal
Toddlers often resist going to bed when their parents want them to go. Parents may have difficulty recognizing whether the resistance is related to true needs and fears or whether it is attention seeking or oppositional. The resistance often takes the form of repeated requests for a snack, a drink, or a trip to the toilet and may include fears of noises, shadows, or imaginary monsters.
A sleep diary can be helpful to sort out the etiology for the sleep refusal and direct management efforts. The parents record bedtimes and waking times for 2 weeks and indicate specific problem behaviors and their responses to each situation. Parents are often able to recognize patterns and problems themselves as they review the diary.
Many common refusal patterns can be addressed by focusing on the problem aspects of good sleep hygiene (Box 24-1). If the problem seems to be oppositional, the best approach is for parents to ignore it. If the child gets out of bed, a parent should place the child back in bed without conversation other than a firm, “It’s time for bed.” When the parents actively ignore their child’s efforts to get attention, the behaviors often get worse before they improve. However, even persistent children eventually respond (Blum and Carey, 1996). If standard ignoring is too stressful on the family, a “gradual ignoring” technique is also effective (Reid et al., 1999) (SOR: B). This involves briefly checking on the child every few minutes until they are asleep and gradually lengthening the interval between checks.
For a child who is fearful, having parents ignore them may make the fears worse. A gradual withdrawal of the parent’s presence after the bedtime routine works better. The parent may sit in the room while the child falls to sleep but should avoid lengthy discussion of the child’s fears. Once the child is able to get to sleep without fear, the parent begins to move their chair closer to the child’s door and eventually outside the bedroom. Fearful children who do not respond to this technique should be considered for referral for more intensive treatment similar to that applied toward phobias.
Night Waking
Most children wake up in the night but are able to get back to sleep without arousing their parents. The exceptions can have a serious impact on the entire family, as previously noted. As with sleep refusal, a sleep diary can help, and parent education regarding good sleep hygiene is beneficial. However, two common problems deserve particular attention: night terrors and nightmares (Table 24-1).
Table 24-1 Diagnostic Features of Night Terrors vs. Nightmares
| Feature | Night Terrors | Nightmares |
|---|---|---|
| Time of night | Early; usually within 4 hours of bedtime | Late |
| State on waking | Disoriented or confused | Upset or scared |
| Response to parents | Unaware of presence; not consolable | Comforted |
| Memory of event | None, unless fully awakened | Vivid recall of dream |
| Return to sleep | Usually rapid, unless fully awakened | Often delayed by fear |
| Sleep stage | Partial arousal from deep non-REM sleep | REM sleep |
REM, Rapid eye movement.
From Blum NJ, Carey WB. Sleep problems among infants and young children. Pediatr Rev 1996; 17(3):87-92.
Night terrors come about as a sudden partial arousal from the deepest non-REM sleep. Essentially, part of the brain snaps into wakefulness, but part remains soundly asleep. Because deep non-REM sleep predominates in the first four hours of sleep, night terrors usually happen during the early part of the night. The child bolts upright in bed, screaming, sweating, tachycardic, and tachypneic. The episodes usually last only a few minutes, ending as abruptly as they began, with the child falling back to sleep quickly unless fully awakened by the parents. Not fully awake, these children do not respond to the parents’ efforts to comfort them. The child appears disoriented and confused, often with a blank stare, and has no recall of the event the next morning. Night terrors usually occur in children ages 2 to 6 years and are more common during times of illness, stress, or sleep deprivation. A nocturnal seizure should be considered in the differential diagnosis if the events are more likely right at sleep onset or if there is a personal or family history of seizures (Dahl, 1998).
Nightmares, on the other hand, are frightening dreams that awaken the child from REM sleep. Therefore, they tend to occur during the second half of the night, leaving the child upset or scared with a vivid recall of the dream. The child responds to comforting efforts by the parent but may be slow to go back to sleep because of fear. As with night terrors, nightmares occur most often during the toddler to preschool years and are more common during stressful times.
Management
In general, sedative medications are not indicated for night waking. Instead, behavior management techniques similar to those outlined for sleep refusal are appropriate for most cases.
There is no specific treatment for night terrors. Parents should be reassured with the explanation that the problem is common and self-limited. They should not try to wake the child up because this may only frighten the child or slow the child’s return to sleep. For children who thrash violently, the parent should take precautions to provide protection for them. If the child sleepwalks into potentially dangerous situations, the parents can hang a bell or electronic movement alarm on the child’s bedroom door to warn them. Because overtiredness is a major factor in the tendency to have night terrors, increasing the total amount of sleep and keeping a consistent sleep-wake cycle should be emphasized.
Because nightmares tend to occur at times of emotional stress, the focus of treatment should be on assisting parents with effective ways to manage the underlying stress. When a nightmare has occurred, the child is awake and frightened. The parent should comfort the child without a detailed review of the nightmare contents or “flashlight searches for monsters” (Blum and Carey, 1996) which can further increase the child’s fears.
Obstructive Sleep Apnea Syndrome
Habitual snoring occurs in 3% to 12% of preschool-age children. The childhood incidence of obstructive sleep apnea syndrome (OSAS) is estimated to be 2%. The American Academy of Pediatrics has published an evidence-based guideline for the diagnosis and management of OSAS (AAP, 2002).
In children, OSAS is most often associated with large adenoids and/or tonsils, as well as specific facial features such as micrognathia, macroglossia, and Down syndrome. Unlike adults with sleep apnea, children can be affected without large drops in blood oxygen levels, because children can have frequent brief awakenings to quickly reestablish their airway. Thus, the primary clinical issue may be sleep fragmentation. In the context of a child with snoring and restless sleep, OSAS should be considered any time there are symptoms or signs suggesting sleep deprivation, such as difficulty paying attention, emotional lability, partial arousals during the night (night terrors, sleepwalking), or difficulty waking up in the morning (Dahl, 1998).
Because only a portion of children with snoring and adenotonsillar hypertrophy have OSAS, a sleep study is recommended to avoid unnecessary surgery. A caution, however, is that sleep studies in children require special expertise that may not be available at an adult sleep center.
Treatment of a child with OSAS on the basis of adenotonsillar hypertrophy is surgery. Continuous positive airway pressure (CPAP) is effective in children but is reserved for when adenotonsillectomy is contraindicated or unsuccessful (AAP, 2002) (SOR: A).
Sleep Deprivation and Delayed Sleep-Phase Syndrome
Sleep deprivation and delayed sleep-phase syndrome are common problems in adolescents for several reasons. The total sleep requirement is as much or more in adolescence as in pre-adolescence (Carskadon and Roth, 2000), but adolescents tend to receive less sleep for both biologic and cultural reasons. School-age children are more likely to be “larks,” preferring to wake up early even if they are up late at night. At puberty, a circadian rhythm change occurs that results in a switch from larks to “owls,” the preference for a late-night bedtime and late-morning awakening. This biologic tendency is encouraged by the availability of stimulating activities late into the night, whether social events, part-time jobs, or technologic advances (e.g., TV, Internet). Stimulants such as caffeine and tobacco also act to delay sleep. Despite these factors that act to delay sleep, school schedules often require the adolescent to awaken early. Thus, sleep deprivation develops. Also, jet lag–like shifts often develop between the weekday and weekend or holiday schedule. These schedule shifts probably play a role in the most common adolescent sleep problem, delayed sleep-phase syndrome (Dahl, 1998).
The assessment is by history. The main differential diagnosis to consider from delayed sleep-phase syndrome is the teenager who is choosing a late-night schedule for some secondary gain. This person is not distressed by the dysfunctional sleep pattern and is unmotivated to change it. Therefore, the adolescent with secondary gain requires treatment directed at the underlying school or family issues rather than the sleep disturbance.
Treatment of the cooperative adolescent involves attempting a schedule shift and consistently maintaining it. Those with marked difficulty initiating timely sleep may respond to staying awake through an entire night, then reestablishing a regular schedule. Mindell and Owens (2009) provide a practical clinical guide for pediatric sleep.
Narcolepsy
Although rare, narcolepsy is an important cause of daytime sleepiness because it can affect personal safety and school performance but is readily treatable. Normally, REM sleep only occurs when a person has been asleep for 60 to 90 minutes and follows all four stages of non-REM sleep. Narcoleptic patients, on the other hand, experience sudden episodes of REM sleep in the middle of a wakeful state or immediately after falling asleep.
The key feature of narcolepsy is recurrent sleep attacks: sudden, unintentional, irresistible bouts of sleep that occur in inappropriate situations, such as during conversations or while driving. Other common findings include cataplexy (sudden bilateral loss of muscle tone without loss of consciousness), hypnagogic hallucinations (vivid dreamlike imagery just before falling asleep), and sleep paralysis (inability to move or speak just after morning awakening). Any child or adolescent with unexplained daytime sleepiness who does not respond to initial management with good sleep hygiene, or who has a family history of narcolepsy, should be considered for evaluation. A sleep study is required to make the diagnosis.
Narcolepsy treatment combines behavioral approaches with medications. The patient should adhere to good sleep hygiene. Therapeutic naps enhance daytime alertness and reduce the necessary dose of stimulants. Stimulant medications, such as methylphenidate, dextroamphetamine, or modafinil are very helpful for daytime sleepiness (Vgontzas and Kale, 1999) (SOR: A). The antidepressants are REM suppressants that help prevent cataplexy or hypnagogic hallucinations. The nonsedating antidepressants, especially the selective serotonin reuptake inhibitors (SSRIs), work synergistically when combined with stimulants (Vgontzas and Kale, 1999) (SOR: B).
Autism
The term autism refers to a spectrum of pervasive developmental disorders characterized by various degrees of impaired social interaction and communication and repetitive, stereotyped patterns of behavior. Patients may have relatively good skills in one area and very poor skills in others. The specific diagnosis of “autistic disorder” has an onset before 3 years of age and requires the presence of impairments in all three categories, whereas “Asperger’s disorder” includes impaired social interaction and autistic behaviors but excludes language delay. The incidence of autistic disorder is 5 to 20 per 10,000 persons, with a much higher occurrence among siblings of affected patients (3%-7%) (Schaefer and Mendelsohn, 2008). Mental retardation, typically in the moderate range (IQ 35-50), accompanies the disorder in 75% of affected children (DSM-IV-TR, 2000).
Evidence is mounting that both genetic and environmental factors influence the etiology of autism (Kolevzon 2007; Schaefer and Mendelsohn, 2008). Assertions that autism is caused by thimerosal-containing vaccines have been discounted by a comprehensive meta-analysis (Parker et al., 2004) (SOR: A).
Assessment
Developmental screening should be part of each well-child examination. The Denver Developmental Screening tools have often been used for this purpose but they lack sensitivity and specificity for autism. The AAP provides a thorough examination of screening instruments for autism (Johnson and Myers, 2007). A variety of screening tools aimed specifically at autism are available but also lack sensitivity (Bryson et al., 2003). Therefore, physicians should take parental concerns about delayed speech and language development seriously, especially beyond 18 months of age, even in the context of normal screening. In addition to delayed speech development, the other common presenting symptom is challenging behavior. The behaviors may include a violent reaction to minor changes in the environment or routine, stereotypic movements such as clapping or rocking, and preoccupation with narrow interests or inanimate objects.
When autism is suspected, a thorough evaluation should be performed, including appropriate intellectual testing, speech-language assessment, Autism Diagnostic Interview–Revised (ADI-R) (Western Psychological Services [WPS], 2003) and the Autism Diagnostic Observation Schedule (ADOS) (WPS, 2001). Because hearing loss can mimic autism, the evaluation should also include formal audiologic testing. Common comorbidities include anxiety, depression, and obsessional behavior (Prater and Zylstra, 2002). Many autistic patients develop infantile spasms in the first year of life, a severe seizure disorder.
Management
Early intervention is important because the younger children are treated, the better the outcome. The most successful programs utilize a multidisciplinary approach that includes behavior modification, development of social communication, active involvement of parents and families, and use of psychotropic medications for dangerous behaviors that do not respond to behavior modification (Myers et al., 2007). Referral to an established program is recommended. Despite anecdotal reports of efficacy of alternative and complementary treatments, none of these has shown benefit in clinically controlled trials. Less than 5% of autistic people become self-sufficient adults, although one-third achieve some degree of independent living (Prater and Zylstra, 2002). Clear gain in language is the most important predictor of adult outcomes (Bryson et al., 2003)
Attention-Deficit/Hyperactivity Disorder
Attention-deficit/hyperactivity disorder (ADHD) is the most frequently diagnosed behavioral disorder of childhood, with a prevalence of 4% to 12% (DSM-IV-TR, 2000). At least 10% of behavior problems seen in a general pediatric practice are caused by ADHD. Boys are seen more frequently than girls. ADHD should be considered and assessed in a child who presents with inattention, hyperactivity, impulsivity, academic underachievement, or behavior problems (AAP, 2000; AHCPR, 1999). ADHD is a chronic disorder persisting from childhood into adolescence and adulthood. In general, symptoms decrease by half every 5 years between ages 10 and 25 (Goldman et al., 1998). Obvious hyperactivity disappears while inattention persists.
Research suggests that ADHD has a central nervous system (CNS) basis; however, no specific etiology has been discovered. Family genetic studies have shown up to 92% concordance in monozygotic twins and 33% concordance in dizygotic twins. Clinicians should keep in mind that the child’s parents may also have ADHD. Various brain imaging studies of ADHD patients have demonstrated abnormalities of brain metabolism, supporting the validity of ADHD as a disorder. However, the strongest evidence of validity has been course prediction and treatment response to medication.
Comorbidity is common in ADHD; 65% of children diagnosed with ADHD have more than one psychiatric diagnosis (Biederman et al., 1991), including about 30% with more than one comorbid condition. Of children diagnosed with ADHD, 35% also have oppositional defiant disorder; 25% have conduct disorder; 18% have a depressive disorder; 25% have an anxiety disorder; and 12% to 60% have a learning disorder (AHCPR, 1999).
Assessment
There is no independent valid test to determine that a child has ADHD. The diagnosis can only be obtained reliably by using well-established diagnostic assessment methods. This involves using the standardized diagnostic criteria of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; Box 24-2), rather than the clinical description of the World Health Organization’s International Classification of Diseases (ICD-9) (AHCPR, 1999). Unfortunately, only 30% of family physicians routinely use the DSM criteria (Rushton et al., 2004). This must be part of a comprehensive diagnostic evaluation that involves obtaining information from the parents, child, and teacher. The baseline assessment of target ADHD symptoms can be assisted by using standardized behavior reports, such as the Conners Rating Scales (1997 revision), NICHQ Vanderbilt forms, or the SNAP checklist. Broadband behavioral rating scales, such as the Child Behavior Check List (CBCL, Achenbach), do not effectively discriminate between ADHD and non-ADHD children but do assist in identifying comorbid disorders (AAP, 2000). Because of the significant prevalence of comorbid psychiatric disorders, the assessment should include inquiring about these conditions (AHCPR, 1999). In addition to psychiatric symptoms, the ability of the child to function normally in different domains must also be assessed. These domains include family relationships with adults, sibling relationships, peer social relationships, community behavior, school academic performance, school behavior, interests and play activities, and subjective psychological distress.
Box 24-2 DSM-IV-TR Diagnostic Criteria For Attention-Deficit/Hyperactivity Disorder
From American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed, Text Revision (DSM-IV-TR). Washington, DC, American Psychiatric Association, 2000.
A. Either (1) or (2)
The physician should conduct a medical screening examination, including hearing and vision tests, if this has not already been done. Other diagnostic tests, including laboratory screening tests for lead intoxication, abnormal thyroid function, neuroimaging for brain tumor, or seizure disorder, should be conducted when indicated by the history and physical examination (AHCPR, 1999). Computerized continuous performance tests should not be used as a clinical screening or diagnostic tool for ADHD.
Management
The clinician should establish a comprehensive management program that recognizes ADHD as a chronic condition and works with the parents, child, and teachers to identify the most important problems as targets of treatment (AHCPR, 1999). Indications for referral to a specialist include (1) children with ADHD plus a comorbid psychiatric disorder and (2) children with ADHD who do not respond to initial treatment. More specific guidance in assessment and management may be obtained by consulting practice guidelines or parameters (AAP, 2000; McDonagh et al., 2009; Pliszka et al., 2007) and health care guidelines (Moore, 2007; O’Brien, 2005). An initial effort must be made to educate the parents and child about ADHD (see Web Resources).
Psychosocial Therapy
The physician or staff should review techniques of parent behavioral management to assess how well they are understood and effectively implemented. This includes the proper use of positive reinforcers and punishment. A structured and standardized system, called the “token economy,” can be very effective but requires considerable time and effort by the parents. Common mistakes made by parents include too much punishment versus positive reinforcement, too long a delay in receiving a reward, making the system too difficult initially so that the child never achieves success, inconsistent implementation, and poor supervision.
Assessing for proper educational placement is important. At a minimum, the parents should consult with the child’s classroom teacher and confirm close supervision of the child, a structured classroom, good behavioral management, and good communication with parents. If this effort is not sufficient, the parents can request educational accommodations under Section 504 of the 1973 Rehabilitation Act. This federal law provides for special accommodations and services in a person with a chronic handicapping condition, including psychiatric disorder. The request must be accompanied by a physician statement documenting the handicapping condition and directed to the building principal or school district “Section 504 compliance officer.” If this is not enough and the child is failing in one or more subjects, the parents can request a comprehensive evaluation by the Child Study Team for possible Special Education placement (“Other Health Impaired” eligibility condition—Federal Public Law 94-142, currently the Individuals with Disabilities Education Act, IDEA). The request should be in writing and directed to the building principal. The evaluation may take up to 85 school days but could result in an individualized education program (IEP), a description and contract of what special services the school will provide.
For children with ADHD alone, other psychosocial treatments have not been shown to be more effective than aggressive use of stimulant medication, or even to provide an additional benefit (MTA Cooperative Group, 1999). However, psychosocial treatments are beneficial in children with ADHD and other comorbid disorders or those from families with chaotic functioning.
Pharmacotherapy
The stimulants are the medications of first choice at any age (AHCPR, 1999); they do not have a paradoxical reverse effect at puberty. Methylphenidate was also shown to be beneficial for very young children with ADHD through the National Institutes of Mental Health (NIMH) Preschoolers with ADHD Treatment Study (PATS); however, the benefit was not as robust as in older children, and adverse effects were more prominent (Abikoff et al., 2007; Gleason et al., 2007). Table 24-2 provides measures for successful stimulant administration, and Table 24-3 lists specific dosing recommendations. Of ADHD children, 70% show significant improvement on the first trial of a stimulant, and 85% to 90% improve significantly taking at least one of the listed stimulants. When the medication is in effect, motor activity decreases, certain cognitive processes improve, motivation improves, academic performance improves, and oppositional and aggressive behaviors decrease. However, the medication works only for as long as it is given, with no long-lasting or curative effect.
Table 24-2 Keys to Successful Pediatric Stimulant Administration
| Recommendation | Comment |
|---|---|
| Be aggressive with titration of medication. | Increase dose until benefit clearly seen or side effects prevent further dose increases. |
| Frequency of doses: cover the day as much as possible and normalize functioning as much as possible. | Give doses at breakfast, lunch, and after school, depending on duration of benefit of the specific stimulant. |
| Monitor closely the beneficial and adverse effects of medication. | Obtain information from both parents and teachers. Use standardized behavior report.∗ |
| See patients at least every 3 months for maintenance treatment. | Try to head off problems before they develop into serious ones. |
| Consider annual discontinuation of medication to see if it is still needed. | However, this is unnecessary if parents still see a clear worsening when medication wears off. |
∗ For example, NICHQ Vanderbilt Assessment Follow-up forms.
Table 24-3 Stimulant Medications Used in Treatment of Attention-Deficit/Hyperactivity Disorder (ADHD)
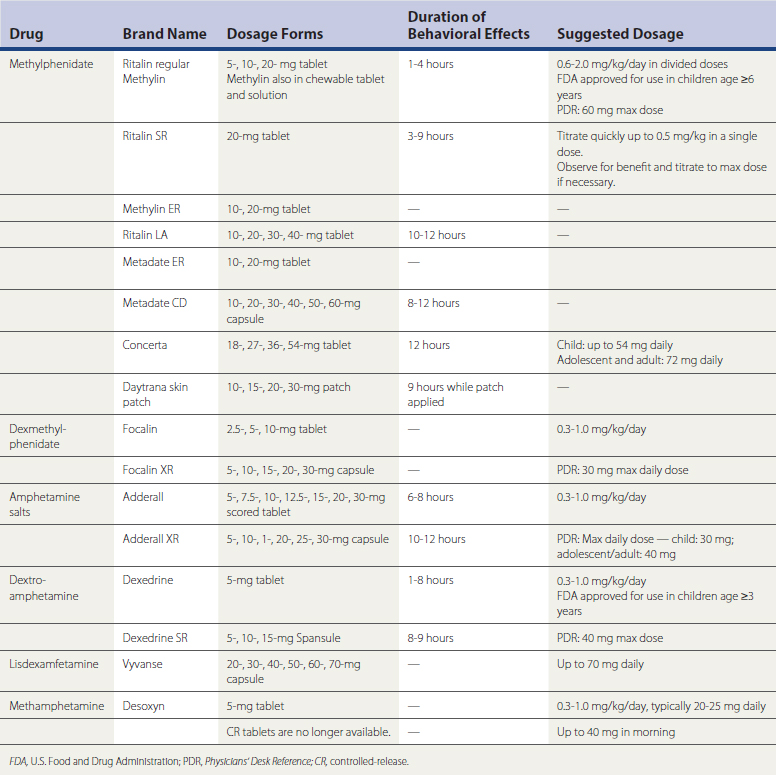
The physician should use a systematic approach. If the first stimulant is not effective after an adequate trial of maximum doses, a sequential trial of each available stimulant is appropriate before moving to another class of medication. At a minimum, at least one methylphenidate preparation and one amphetamine preparation should be tried. Follow-up appointments should be regular and scheduled and should include information from the parents, teachers, and child (AHCPR, 1999). Adverse effects are similar for all stimulants and can affect up to 20% of children. Important side effects include anorexia, weight loss, irritability (more likely in younger children), abdominal pain, insomnia (only if given after 5 pm), dysphoria (more likely in younger children), “behavioral rebound” after wearing off, impaired cognitive performance on laboratory tests (methylphenidate at single doses >1 mg/kg), tachycardia, and increased tic symptoms (if patient has tic disorder). In general, growth suppression is not a concern, except in children with dramatic anorexia. There is no evidence that the legitimate prescribed use of stimulants by ADHD children and adolescents lead to future drug abuse, and proper use may actually have a protective effect. Sudden death in children taking stimulant medication was recently a concern (Gould 2009). The U.S. Food and Drug Administration (FDA) issued a 2009 communication recommending caution but not stopping the use of stimulants for ADHD. A more definitive study involving 500,000 stimulant medication users is expected soon.
The third line of treatment (after two trials of stimulants) is atomoxetine, which has an FDA indication for the treatment of ADHD. It is initially given at 0.5 mg/kg/day, either in the early morning or as a divided dose (morning and late afternoon). It is titrated up to a maximum dose of 1.4 mg/kg/day (or 100 mg maximum). The full benefit may not be seen for 4 weeks (ICSI, 2005). Common adverse effects include nausea, vomiting, gastrointestinal pain, anorexia, headache, fatigue, and sleepiness. Atomoxetine is not a U.S. Drug Enforcement Administration (DEA) scheduled medication, has no potential for abuse, and therefore can be written with refills.
Bupropion, tricyclic antidepressants (TCAs, e.g., imipramine, nortriptyline), and the alpha-adrenergic agent clonidine do not have an official FDA indication for the treatment of ADHD. The evidence for their benefit is based on randomized controlled trials (RCTs) and nonrandomized trials with controls (ICSI, 2007). Two alpha agents, guanfacine and clonidine, in extended-release forms, have received FDA approval for treatment of ADHD. Further information can be found by referring to the Texas Children’s Medication Algorithm Project (most recent algorithms, May 2006; see Web Resources), developed by expert consensus (Pliszka 2000). Atypical antipsychotic medication (i.e., risperidone), mood stabilizers (lithium, valproic acid), or clonidine can be used in children with comorbid severe aggression or suspected bipolar disorder after an adequate trial of a standard ADHD medication (Barzman and Sorter, 2009).
Oppositional Defiant Disorder
Key PointsThe prevalence of oppositional defiant disorder (ODD) in children under 18 years old is widely reported as 2% to 16%. Before puberty, males outnumber females, but after puberty the rates are more equal. The disorder is usually evident by 8 years of age (APA, 2000). ODD is a chronic persistent disorder; however, approximately 67% of childhood cases have resolved 3 years later. About 30% of children with early-onset ODD develop conduct disorder (Connor et al., 2002).
The characteristics predisposing to ODD are biologic, social, and psychological, involving the parents and child. The parents usually employ poor, ineffective, inconsistent, and indiscriminate behavioral management methods, which are often combined with unusually harsh but inconsistent discipline and poor monitoring of activities. These children are usually temperamental, impulsive, active, and inattentive. The parents themselves are frequently immature, temperamental, and impulsive. The family members usually experience significant marital, financial, health, and personal distress (Barkley, 1997).
Assessment
There are two periods of developmentally normal oppositional behavior: the “terrible twos,” between 18 and 24 months of age, when the toddler behaves negatively as an expression of developing autonomy, and sometimes in adolescence, when the teenager is trying to separate from the parents and establish an autonomous identity. Unlike ODD, these stages usually last less than 6 months (see eBox 24-1).
A child with ODD reported by the parents may not show much oppositional behavior while being examined in the office. The symptoms of ODD that these children display are much more evident in interactions with people and situations that they know well. The child takes a self-defeating position in arguments with adults. The struggle becomes more important than the reality of the situation, such that the child may be willing to risk losing the object or activity rather than lose the argument. Even a significant delay by the child in complying with a parental request is seen as a victory by the child. The assessment of ODD should include direct information from the child and parents regarding symptoms, age of onset, duration, and degree of functional impairment.
If oppositional behavior is confined mostly to school and not much at home (except as it relates to schoolwork), additional diagnoses must be considered in the differential, including mental retardation, borderline intellectual functioning, a specific developmental disorder (e.g., learning disability), and most often, ADHD. No specific laboratory tests or pathologic findings can assist the clinician in making the specific diagnosis of ODD.
Management
With methodologically sound RCTs lacking and recommendations based on clinical consensus, the appropriate psychosocial interventions for ODD include parenting training in behavior management techniques: improved parent/child relationship, positive reinforcement, closer supervision, giving more effective commands, time-out, and token economies. Despite the usually chaotic family situation and high emotions involved, the family physician needs to establish a therapeutic alliance with both the child and the family to have the best chance of success (Steiner and Remsing, 2006). Interventions should be family based, targeted to specific concerns, and oriented to problem solving. Traditional individual psychotherapy, unstructured/nondirected family therapy, or short-term treatment is usually not helpful. Psychoactive medications are used to treat comorbid conditions and targeted symptoms but have not demonstrated benefit for ODD alone. Intense and prolonged treatment may be necessary for severe and persistent ODD. One-time crisis interventions (e.g., “scared straight” attempts) are not effective.
Conduct Disorder
Key PointsThe prevalence of conduct disorder (CD) in children under 18 years old is 6% to 16% in males and 2% to 9% in females. At all ages, boys outnumber girls. Males usually exhibit more aggression, whereas females usually commit more covert crimes and prostitution. CD is more common in urban than rural settings and is one of the most frequent diagnoses in outpatient and inpatient psychiatric facilities for children. The mortality rate for seriously disturbed delinquents is 50 times higher than for normal youths. Adolescents with CD are more likely to die by homicide, suicide, violent accident, or drug overdose.
Generally, the natural history of children with severe CD is marked by the development of ADHD at a very early age, followed by ODD, then finally the onset of CD. In adolescence, alcohol and substance abuse occur. The factors that determine a poorer prognosis in the patient with CD are an early age of onset of symptoms, greater number of symptoms, and greater frequency of expression of these CD symptoms. The factors that determine a better prognosis are minimum number of CD symptoms, absence of comorbid psychiatric diagnoses, and normal intellectual functioning. Characteristics more common in childhood-onset versus adolescent-onset CD are greater frequency of neuropsychiatric disorders, lower IQ, higher levels of aggression, male gender, and greater frequency of externalizing behavior disorders in other family members. From 25% to 40% of children with CD go on to develop antisocial personality disorder, a chronic pattern of lawlessness.
Current views posit an interaction among genetic, biologic, and environmental factors (i.e., parental, sociocultural, psychological, prolonged abuse). No single factor accounts for more than 50% of the variance in the occurrence of CD, and no combination of factors accounts for more than 70% of the variance. Many children with risk factors do not develop CD.
Assessment
The diagnostic criteria for CD are summarized in eBox 24-2. The clinician should not quickly accept the diagnosis of CD in a youth, because no specific effective treatment exists, and instead should diligently search for other, more treatable psychiatric conditions. Other psychiatric diagnoses that should be considered as the primary disturbance in a child presenting with CD symptoms include ADHD, ODD, intermittent explosive disorder, psychoactive substance use disorder, mood disorders (bipolar and depressive disorders), posttraumatic stress disorder (PTSD), dissociative disorder, borderline personality disorder, and adjustment disorder with disturbance of conduct. A manic episode must be seriously considered in a teenager presenting with frequent lying, physical aggression against others, impulsive sexual activity, stealing, sneaking out in the middle of the night, grandiosity, and persistent pervasive irritability.
The interview of an adolescent with CD is not sufficient, in itself, for the psychiatric evaluation. Lying is a common problem for these teenagers, as is conscious and unconscious underreporting of their problem behaviors. Other sources of information, including parents, teachers, other professionals, past records, and court personnel, are essential to obtain a valid evaluation. Complications seen in association with CD symptoms include impairment in school performance, poor social and family relationships, problems with the legal system, poor work performance, physical injuries from fighting or carelessness, sexually transmitted diseases, teenage pregnancy, drug problems, suicide, and homicide. Common examples of interpersonal impairment in these children include suspiciousness or paranoia, misperception of others’ actions as hostile, difficulty relating to peers and adults, lack of guilt, and lack of empathy.
Children with CD respond differently to punishment than normal children. The frequency of negative behavior of normal children decreases when they are punished, whereas the negative behavior of children with CD increases when they are punished.
There are no specific laboratory tests that assist in making the diagnosis of CD. However, the differential diagnosis for CD symptoms includes conditions for which tests may be important. These include head trauma, seizure disorder, birth injury to the brain, and encephalitis.
Management
One-time interventions affecting a single domain will be ineffective in treating CD. Interventions need to target all affected domains in a naturalistic setting for a long period in a consistent manner. Family interventions (parenting training/guidance, functional family therapy) and social skill training with a behavioral approach seem to be the most effective treatments for the CD patient (Dillon et al., 2007, Steiner, 1997). The focus should be on the child and the family. Individual therapy that focuses on problem-solving skills can also be useful. An environment with consistent rules and consequences is helpful. Proper school placement using behavioral techniques to encourage prosocial behavior and discourage antisocial incidents is appropriate.
Factors that can cause a cognitive-behavioral treatment program to fail include the following: the situation is “too hot to handle”; the youth is “too brittle”; the parents covertly support the youth’s behavior; the parents have given up on the youth; the parents are inconsistent and are unable to supervise adequately; the program is poorly designed; rewards are too costly; or the parents have little social support. Factors that can interfere with limit setting of the child or adolescent at home include parental conflict, parental absence, parental psychiatric illness, inconsistent discipline, and vague or minimal expectations regarding appropriate behavior.
Several legal options are available if parents are unable to control their children. Most state laws have a special status that can be petitioned by the county district attorney to the juvenile court judge (i.e., Child/Person in Need of Care laws), that can allow the court to supervise the child by having hearings, placing a child on probation, mandating treatment and monitoring, or eventually taking the child away from the parents and placing the child in a residential treatment facility. However, some dangers must be kept in mind when teenagers with CD are confined to a juvenile detention facility. These patients prefer to be unrestricted and active; they can become depressed and at risk for impulsively attempting suicide when placed in confinement. Inpatient psychiatric hospitalization can be used to assess and initiate treatment for comorbid psychiatric disorders. A homicidal or suicidal patient can be stabilized and then moved to a less restrictive long-term setting. However, the stay is usually too brief to effectively treat CD itself.
Medications used as the sole treatment for conduct disorder have not been demonstrated to be effective. Psychoactive medications are used for the treatment of concurrent psychiatric disorders and concurrent target symptoms (aggression, impulsiveness, mood instability). Some of these medications are lithium, antidepressants, carbamazepine, propranolol, stimulants, clonidine, and antipsychotics (usually haloperidol). The physician should be cautious when prescribing medication to a youth with CD. Medication can be “cheeked,” sold or traded, hoarded, and taken all at once in an impulsive suicide attempt.
Eating Disorders
Key PointsThe most common and most serious eating disorders, anorexia nervosa and bulimia nervosa, typically have their onset in adolescence. However, several eating problems are associated with infants and children as well.
Feeding and Eating Disorders of Infancy and Early Childhood
Feeding difficulties are common in infants and young children. Most are minor and self-limited and can be addressed through education and reassurance of caregivers. However, physicians must be alert for specific feeding and eating disorders that can lead to malnutrition or chronic toxicity from ingested substances. The most important of these are listed in DSM-IV-TR as “Feeding Disorder of Infancy or Early Childhood.” The diagnosis has previously been described as “psychosocial failure to thrive” and “psychosocial dwarfism.” The key feature of the diagnosis is that the child fails to gain weight appropriately over a prolonged time, which is not fully explained by a gastrointestinal, endocrinologic, or neurologic condition. Of children admitted to the hospital for failure to thrive, as many as half have a psychosocial etiology.
The other important consideration in this category is pica, the persistent eating of nonnutritive substances, such as hair, soil, paint, animal droppings, or sand. Pica can result in vitamin deficiencies, lead or other heavy metal intoxication, phytobezoars, and other complications. The prevalence of pica is not certain, but it is probably fairly common in preschool children, especially those with mental impairment.
The most important aspect in assessing feeding difficulties in infants and children is tracking height and weight with each office visit. Children who are not maintaining expected gains should be observed more closely, keeping in mind that a significant proportion of these children have a psychosocial basis. The diagnosis of feeding disorder is suggested by improvement in feeding and weight gain following a change in caregivers. When a diagnosis of feeding disorder is entertained, consultation with a physician familiar with growth problems in children should be considered, because the differential diagnosis for growth problems is extensive, and diagnostic implications include child abuse and neglect.
The important aspect to assessment of pica is to ask. Evaluation and treatment then depend on the specific substance ingested and symptoms the child exhibits, if any.
Anorexia Nervosa and Bulimia Nervosa
In adolescent girls, eating disorders are the third leading chronic illness, after obesity and asthma. The number of young people diagnosed with eating disorders (anorexia nervosa or bulimia nervosa) and eating disturbances (some but not all criteria for diagnosis of a “disorder”) is increasing, the result of a combination of improved recognition and reporting, as well as an apparent true increased incidence. About 95% of cases are female, and the prevalence of eating disorders has been directly correlated to the rates of dieting behavior. High-risk groups include female athletes and diabetic patients.
An individual with anorexia nervosa refuses to maintain a minimally normal body weight, is fearful of gaining weight, and exhibits a distorted body self-image. If she is postmenarchal, she is amenorrheic. The long-term mortality rate for anorexia nervosa is 6% to 20%, the highest rate for any psychiatric disorder (Roerig et al., 2002), often as an acute suicidal act rather than slow bodily destruction alone (Pompili et al., 2006). Bulimia nervosa is characterized by binge eating and inappropriate compensation attempts to avoid weight gain, such as self-induced vomiting, misuse of laxatives or diuretics, fasting, or excessive exercise. The prevalence of bulimia nervosa is 1% to 3% in adolescent and young adult women, more common but less often fatal than anorexia nervosa (DSM-IV).
Assessment
A prime objective in assessment is to distinguish “normal dieters” from individuals with eating disorders. In addition to the characteristics outlined in Table 24-4, patients with eating disorders have a pathologic reaction to weight gain. To explore this possibility, a useful question to ask is, “What would it be like to find you weighed one pound more next week when you get on the scales?” This may provoke an overly emotional response in a person with an eating disorder (Selzer et al., 1995).
Table 24-4 Characteristics of Normal Dieting vs. Eating Disorders
| Feature | Normal dieting | Eating disorder |
|---|---|---|
| Communication with others | Dieters tell those around them that they are dieting, seeing it as “something to be proud of.” | Dieters are reluctant to discuss their diets even when it is obvious to those around them that they are restricting their intake. |
| Intake regulation | They use internal cues and the rules of their diet plan. | They often use external cues, such as eating less than the person at the table who eats the least, to avoid feeling selfish or gluttonous. |
| Behavior | When weight loss goal achieved, they want to show off their “new body,” often in new and more revealing clothes or situations (e.g., new swimsuit, sunbathing). | They usually avoid exposing their bodies, often with baggy clothing, or regard their physical dimensions with disgust, no matter how much weight they lose. |
| Self-esteem | They exhibit a feeling of accomplishment and increased self-esteem when they achieve planned weight loss. | They tend to become self-critical, often depressed or irritable, and avoid social occasions. |
Another important aspect to evaluation is to exclude certain medical conditions in the differential diagnosis as the primary cause of the symptoms. This includes such diverse problems as inflammatory bowel disease, hyperthyroidism, chronic infections, diabetes mellitus, and Addison’s disease. The erythrocyte sedimentation rate (ESR) and serum albumin tend to remain normal in patients with eating disorders, so an elevated ESR or a reduced albumin suggest an organic cause for weight loss (Selzer et al., 1995).
It is important to assess the acuteness and severity of malnutrition or fluid and electrolyte abnormalities. Indications for immediate referral include any patient with abnormal findings on physical examination or laboratory studies because these indicate severe and entrenched eating disorders. Laboratory studies should include a complete blood count, electrolytes, magnesium, calcium, phosphorus, urea nitrogen, creatinine, glucose, albumin, and electrocardiogram (Walsh et al., 2000).
Extreme weight loss is difficult to define in growing adolescents. The usual criteria of less than 85% of average body weight (ABW) and body mass index (BMI) less than 17.5 kg/m2 used to diagnose anorexia nervosa in adults can be misleading. The most clinically useful measure is BMI percentile adjusted for age (Hebebrand et al., 1996). A reading less than the fifth percentile is considered extreme (Selzer et al., 1995). Finally, for anorexia nervosa, the presence of vomiting is a poor prognostic feature, as is the use of purgatives for bulimia nervosa (Wilhelm and Clarke, 1998).
Management
Indications for inpatient management include “extremely low weight (≤75% of expected body weight) or rapid weight loss; severe electrolyte imbalances, cardiac disturbances, or other acute medical disorders; severe or intractable purging; psychosis or a high risk of suicide; and symptoms refractory to outpatient treatment” (Becker et al., 1999).
Patients with eating disorders should be managed by a multidisciplinary team that includes a primary physician, mental health professional, and nutritionist. Family physicians should be aware of the resources available in their area and should be prepared to refer any adolescent suspected of an eating disorder or with abnormal eating behaviors who does not respond to initial efforts at diet education. A valuable resource for developing a treatment plan is a practice guideline published by the American Psychiatric Association (Yager, APA Work Group, 2006).
Various antidepressants are effective for treatment of bulimia nervosa but have not shown definite benefit for anorexia nervosa. Cognitive-behavioral therapy has been shown to be the most effective psychological approach to bulimia nervosa (Berkman et al., 2006).
KEY TREATMENT
www.dshs.state.tx.us/mhprograms/adhdpage.shtm Texas Children’s Medication Algorithm Project; most recent algorithms May 2006.
www.nlm.nih.gov/medlineplus/sleepdisorders.html National Institutes of Health (NIH)–sponsored patient-oriented site with extensive background information and links to recent research and ongoing clinical trials.
www.sleepfoundation.org/ Sponsored by the National Sleep Foundation, an advocacy group; a patient-oriented site with direct answers to frequently asked questions.
www.aasmnet.org/ Sponsored by the American Academy of Sleep Medicine, a professional society, with public access to patient information and referral centers.
www.ninds.nih.gov/disorders/autism/detail_autism.htm NIH-sponsored patient-oriented site with extensive background information and links to other valuable sites.
www.autism-society.org Sponsored by the Autism Society of America, a national advocacy group, with good general information and networking opportunities.
www.lpch.org/diseaseHealthInfo/healthLibrary/growth/encopres.html Sponsored by the Lucile Packard Children’s Hospital at Stanford, answers patients’ frequently asked questions, including diet and activity recommendations.
http://familydoctor.org/online/famdocen/home/children/parents/toilet/366.html Sponsored by the AAFP, with general patient recommendations; less commercialized than many other sites.
Attention-Deficit/Hyperactivity Disorder
www.chadd.org/ Resources from the national support group for children and adults with ADHD.
www.nichq.org/adhd_tools.html#adhd_parent Resources for clinicians and parents on ADHD from the National Initiative for Children’s Healthcare Quality, including a number of assessment forms.
www.add.org/ Resources from the ADD Association, a national ADHD adult support group.
www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml Information on ADHD from the National Institutes of Mental Health, including a link to current ADHD clinical trials.
Oppositional Defiant and Conduct Disorders
www.aacap.org/cs/ODD.ResourceCenter Resource Center on ODD by the American Academy of Child and Adolescent Psychiatry.
http://jamesdauntchandler.tripod.com/ODD_CD/oddcdpamphlet.htm Detailed assessment and treatment information on ODD and CD from a physician; includes case examples.
www.adhd.com.au/conduct.html Information on CD from an Australian clinic.
www.nationaleatingdisorders.org Sponsored by the National Eating Disorders Association, an advocacy group, with general information and networking opportunities.
www.anad.org Sponsored by the National Association of Anorexia Nervosa and Associated Eating Disorders, an advocacy group with general information and networking opportunities.
Abikoff H.B., et al. Methylphenidate effects on functional outcomes in the Preschoolers with Attention-Deficit/Hyperactivity Disorder Treatment Study (PATS). J Child Adolesc Psychopharmacol. 2007;17:581-592.
Agency for Healthcare Policy and Research (AHCPR). Diagnosis of attention-deficit/hyperactivity disorder. Technical Review No. 3, 1999.
American Medical Association (AMA). Council on Scientific Affairs (A-05) Report 10. Safety and efficacy of selective serotonin reuptake inhibitors (SSRIs) in children and adolescents, August 2005.
American Academy of Pediatrics (AAP). Clinical practice guideline: diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder (AC0002). Pediatrics. 2000:105:1158-1170 . http://aappolicy.aappublications.org/cgi/reprint/pediatrics;105/5/1158.pdf Accessed January 2010
AAP. Clinical practice guideline: treatment of the school-aged child with attention-deficit/hyperactivity disorder. Pediatrics. 2001:108:1033-1044 . http://aappolicy.aappublications.org/cgi/reprint/pediatrics;108/4/1033.pdf Accessed January 2010
AAP, Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002:109:704-712 . http://aappolicy.aappublications.org/cgi/reprint/pediatrics;109/4/704.pdf Accessed January 2010
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: APA; 2000. text revision (DSM-IV-TR).
Barkley R.A. Defiant Children: a Clinician’s Manual for Assessment and Parent Training, 2nd ed. New York: Guilford Press; 1997. :39-40
Barzman D., Sorter M. Best Evidence Statement (BESt): Pharmacological treatment of aggression in children with attention deficit hyperactivity disorder (ADHD). 2009. Cincinnati Children’s Hospital Medical Center http://www.cincinnatichildrens.org/assets/0/78/1067/2709/2777/2793/9198/81559498-09b8-4517-be39-96af49871cdf.pdf. Accessed January 2010
Becker A.E., Grinspoon S.K., Klibanski A., Herzog D.B. Eating disorders. N Engl J Med. 1999;340(14):1092-1098.
Berkman ND, Bulik CM, Brownley KA, et al. Management of eating disorders. Evidence Report/Technology Assessment No 135. AHRQ Pub No 06–E010. April 2006.
Biederman J., Newcorn J., Sprich S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am J Psychiatry. 1991;148:564-577.
Blum N.J., Carey W.B. Sleep problems among infants and young children. Pediatr Rev. 1996;17:87-92.
Borowitz S.M., Cox D.J., Sutphen J.L., Kovatchev B. Treatment of childhood encopresis: a randomized trial comparing three treatment protocols. J Pediatr Gastroenterol Nutr. 2002;34:378-384.
Brazzelli M., Griffiths P.V. Behavioral and cognitive interventions with or without other treatments for the management of faecal incontinence in children. Cochrane Database Syst Rev. 2006;2:CD002240.
Bryson S.E., Rogers S.J., Fombonne E. Autism spectrum disorders: early detection, intervention, education, and psychopharmacological management. Can J Psychiatry. 2003;48:506-516.
Carskadon M., Roth T. Adolescent Sleep Needs and Patterns: Research Report and Resource Guide. 2000. National Sleep Foundation http://www.sleepfoundation.org/sites/default/files/sleep_and_teens_report1.pdf. Accessed January 2010
Connor D.F., Glatt S.J., Lopez I.D., et al. Psychopharmacology and aggression. I. A meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry. 2002;41:253-261.
Dahl R.E. The development and disorders of sleep. Adv Pediatr. 1998;45:73-90.
Dillon A., et al. Parent-education training programmes in the management of children with conduct disorders. 2007. National Institute for Health and Clinical Excellence http://guidance.nice.org.uk/index.jsp?action=download&o=33427. Accessed January 2010
Elia J., Ambrosini P., Rapoport J.L. Treatment of attention-deficit-hyperactivity disorder. N Engl J Med. 1999;340:780-788.
Fabiano G.A., Pelham W.E.Jr., Coles E.K., et al. A meta-analysis of behavioral treatments for attention-deficity/hyperactivity disorder. Clin Psychol Rev. 2009;29:129-140.
Farley S.E., Adams J.S., Lutton M.E., et al. What are effective treatments for oppositional and defiant behaviors in preadolescents? J Fam Pract. 2005;54:162-165.
FDA, FDA. See US Food and Drug Administration.
Fingeret M.C., Warren C.S., Cepeda-Benito A. Eating disorder prevention research: a meta-analysis. Eating Disorders. 2006;14:191-213.
Fombonne E. Increased rates of psychosocial disorders in youth. Eur Arch Psychiatry Clin Neurosci. 1998;248:14-21.
Glazener C.M.A., Evans J.H.C. Desmopressin for nocturnal enuresis in children. Cochrane Database Syst Rev. 2002:3.
Glazener C.M.A., Evans J.H.C., Peto R.E. Complex behavioral and educational interventions for nocturnal enuresis in children. Cochrane Database Syst Rev. 2004;1:CD004668.
Glazener C.M.A., Evans J.H.C., Peto R.E. Alarm interventions for nocturnal enuresis in children. Cochrane Database Syst Rev. 2005;2:CD002911.
Gleason M.M., et al. Psychopharmacological treatment for very young children: contexts and guidelines. J Am Acad Child Adolesc Psychiatry. 2007;46:1532-1572.
Goldman L.S., Genel M., Bezman R.J., Stanetz P.J. Diagnosis and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Council on Scientific Affairs, American Medical Association. JAMA. 1998;279(14):1100-1107.
Gould M.S., Walsh B.T., Munfakh J.L., et al. Sudden death and use of stimulant medications in youth. Am J Psychiatry. 2009;166:992-1001.
Green M., Wong M., Atkins D., et al. Diagnosis of attention-deficit/hyperactivity disorder. Technical Review No 3. 1999 Rockville, Md:US Department of Health and Human Services, Agency for Health Care Policy and Research . http://www.ahcpr.gov/clinic/epcsums/adhdsutr.htm, AHCPR Pub 99-0050. Accessed January 2010
Greenhill L.L., et al. Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry. 2002 :41(Suppl), http://www.aacap.org/galleries/PracticeParameters/JAACAP%20Stimulant%20meds%202002.pdf Accessed January 2010
Guntheroth W.G., Spiers P.S. Sleeping prone and the risk of sudden infant death syndrome. JAMA. 1992;267(17):2359-2362.
Hagglof B., Andren O., Bergstrom E., et al. Self-esteem in children with nocturnal enuresis and urinary incontinence: improvement of self-esteem after treatment. Eur Urol. 1998;33(Suppl 3):16-19.
Hammerness P., McCarthy K., Mancuso E., et al. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder in children and adolescents: a review. Neuropsychiatr Dis Treat. 2009;5:215-226.
Hebebrand J., Himmelmann G.W., Heseker H., et al. Use of percentiles for the body mass index in anorexia nervosa: diagnostic, epidemiological, and therapeutic considerations. Int J Eat Disord. 1996;19:359-369.
Hjalmas K. Nocturnal enuresis: basic facts and new horizons. Eur Urol. 1998;33(Suppl 3):53-57.
Hughes C.W., Emslie G.J., Crismon M.L., et al. The Texas Children’s Medication Algorithm Project: Report of the Texas Consensus Conference Panel on Medication Treatment of Childhood Major Depressive Disorder. J Am Acad Child Adolesc Psychiatry. 1999;38:1442-1454.
Institute of Clinical Systems Improvement (ICSI). Health care guideline: ADHD. Attention deficit hyperactivity disorder in primary care for school-age children and adolescents: diagnosis and management, 2005.
Ipser J., Stein D.J. Systematic review of pharmacotherapy of disruptive behavior disorders in children and adolescents. Psychopharmacology (Berl). 2007;191:127-140.
Jesner O.S., Aref-Adib M., Coren E. Risperidone for autism spectrum disorder. Cochrane Database Syst Rev. 2007;1:CD005040.
Johnson C.P., Myers S.M. Identification and evaluation of children with autism spectrum disorders. Pediatrics. 2007:120:1183-1215 . http://pediatrics.aappublications.org/cgi/reprint/peds.2007-2361v1?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&fulltext=autism&andorexactfulltext=and&searchid=1&FIRSTINDEX=0&sortspec=relevance&resourcetype=HWCIT Accessed January 2010
Johnson L.A., Safranek S., Friemoth J. What is the most effective treatment for ADHD in children? J Fam Pract. 2005;54:166-168.
Kiddoo D., Klassen T.P., Lang M.E., et al. The effectiveness of different methods of toilet training for bowel and bladder control. Evidence Report/Technology Assessment No 147. University of Alberta Evidence-based Practice Center. AHRQ Pub No 07-E003. Rockville, Md: Agency for Healthcare Research and Quality; 2006.
Kolevzon A., Gross R., Reichenberg A. Prenatal and perinatal risk factors for autism; a review and integration of findings. Arch Pediatr Adolesc Med. 2007;161:326-333.
Mahajan P., Pearlman D., Okamoto L. The effect of fluticasone propionate on functional status and sleep in children with asthma and on the quality of life of their parents. J Allergy Clin Immunol. 1998;102:19-23.
McDonagh M.S., Christensen V., Peterson K., Thakurta S. Drug class review on pharmacologic treatments for ADHD. Oregon Evidence-based Practice Center. Final Report, Update. 3 October 2009 http://derp.ohsu.edu/final/ADHD_final_report_update%203_OCT_09.pdf
Mindell J., Owens J. Clinical Guide to Pediatric Sleep: Diagnosis and Management of Sleep Problems, 2nd ed. Lippincott–Williams & Wilkins; 2009.
Moore K. Health care guideline: attention deficit hyperactivity disorder in primary care for school age children and adolescents, diagnosis and management of. Institute for Clinical Systems Integration. 2007 http://www.icsi.org/adhd/adhd_2300.html Accessed January 2010
MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Multimodal Treatment Study of Children with ADHD. Arch Gen Psychiatry. 1999;56:1073-1086.
Myers SM, Johnson CP. Council on Children with Disabilities. Management of children with autism spectrum disorders, Pediatrics 2007;120:1162-1182. http://pediatrics.aappublications.org/cgi/reprint/peds. Accessed January 2010
O’Brien J. Guidelines for clinical care: attention-deficit hyperactivity disorder. 2005. University of Michigan Health System http://cme.med.umich.edu/pdf/guideline/adhd05.pdf. Accessed January 2010
Parker S.K., Schwartz B., Todd J., Pickering L.K. Thimerosal-containing vaccines and autistic spectrum disorder: a critical review of published original data. Pediatrics. 2004;114:793-804.
Pliszka S.R., et al. The Texas Children’s Medication Algorithm Project. Part II. Tactics. J Am Acad Child Adolesc Psychiatry. 2000;39:920-927.
Pliszka S.R., et al. Practice parameter for the assessment and treatment of children, adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2007:46:894-921 . http://www.aacap.org/galleries/PracticeParameters/JAACAP_ADHD_2007.pdf Accessed January 2010
Pompili M., Girardi P., Tatarelli G., et al. Suicide and attempted suicide in eating disorders, obesity and weight-image concern. Eating Behav. 2006;7:384-394.
Prater C.D., Zylstra R.G. Autism: a medical primer. Am Fam Physician. 2002;66:1667-1673.
Reid M.J., Walter A.L., O’Leary S.G. Treatment of young children’s bedtime refusal and nighttime wakings: a comparison of “standard” and graduated ignoring procedures. J Abnorm Child Psychol. 1999;27:5-16.
Reiff M.I. ADHD: a complete and authoritative guide. American Academy of Pediatrics; 2004.
Roerig J.L., Mitchell J.E., Myers T.C., Glass J.B. Pharmacotherapy and medical complications of eating disorders in children and adolescents. Child Adolesc Psychiatr Clin North Am. 2002;11:365-385.
Rogers S.J., Vismara L.A. Evidence-based comprehensive treatments for early autism. J Clin Child Adolesc Psychol. 2008;37:8-38.
Rosack J. New data show declines in antidepressant prescribing. Psychiatr News. 2005;40:1-39.
Rosen C.L. Sleep disorders in infancy, childhood, and adolescence. Curr Opin Pulm Med. 1997;3:449-455.
Rushton J.L., Fant K.E., Clark S.J. Use of practice guidelines in the primary care of children with attention-deficit/hyperactivity disorder. Pediatrics. 2004:114:e24-e28 . http://www.pediatrics.org/cgi/content/full/114/1/e23
Schaefer G.B., Mendelsohn N.J. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders. Genet Med. 2008;10:301-305.
Selzer R., Bonomo Y., Patton G. Primary care assessment of a patient with an eating disorder. Aust Fam Physician. 1995;24:2032-2036.
Steiner H. Practice parameters for the assessment and treatment of children and adolescents with conduct disorder. J Am Acad Child Adolesc Psychiatry. 1997:36(Suppl 10):122-139 . http://www.aacap.org/galleries/PracticeParameters/JAACAP%20Conduct%20Disorder%201997.pdf Accessed January 2010
Steiner H., Remsing L. practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2006:46:126-141 . http://www.aacap.org/galleries/PracticeParameters/JAACAP_ODD_2007.pdf Accessed January 2010
US Food and Drug Administration. Communication about an ongoing safety review of stimulant medications used in children with attention-deficit/hyperactivity disorder (ADHD), 2009. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm165858.htm. Accessed January 2010
Vgontzas A.N., Kales A. Sleep and its disorders. Annu Rev Med. 1999;50:387-400.
Walsh J.M.E., Wheat M.E., Freund K. Detection, evaluation, and treatment of eating disorders: the role of the primary care physician. J Gen Intern Med. 2000;15:577-590.
Wilhelm K.A., Clarke S.D. Eating disorders from a primary care perspective. Med J Aust. 1998;168:458-463.
Yager J. APA Work Group on Eating Disorders. Practice Guideline for the Treatment of Patients with Eating Disorders. 3rd ed 2006 Chicago:American Psychiatric Association http://www.psychiatryonline.com/pracGuide/loadGuidelinePdf.aspx?file=EatingDisorders3ePG_04-28-06. Accessed January 2010
Encopresis
Key PointsEncopresis is the repeated passage of feces into inappropriate places, such as the clothing or floor, by a child who is developmentally over 4 years of age. The passage of stool is usually involuntary and associated with constipation in the vast majority of cases. Chronic constipation leads to an overflow incontinence of feces. The constipation can also lead to rectal pain and fissures that further worsen fecal retention and thus the encopresis.
Fecal retention can initially develop for a variety of psychological and physiologic reasons. Psychological factors include fears that develop around toilet training or loss of privacy during toileting, as in public places or daycare. Physiologic factors include diet transitions, such as from breast milk to formula or the initiation of cow’s milk in the diet. The occasional cases of encopresis not associated with constipation may be caused by organic disease. When the incontinence is clearly deliberate, it is usually in the context of oppositional defiant disorder or conduct disorder. Encopresis occurs in about 1% of 5-year-olds and is more common in boys than girls (DSM-IV-TR, 2000). It is accompanied by enuresis in more than 40% of cases.
Assessment
The primary goals of evaluation are to assess the presence or absence of constipation in the encopretic child and to identify any serious psychological or pathophysiologic factors that are present. This can be achieved in most cases through a conscientious history and physical examination, including digital rectal exam. An extremely useful tool is a 5-day to 7-day symptom and diet diary. The family is asked to record the frequency and character of the stool and episodes of pain or encopresis. The diet history establishes nutritional adequacy and fiber content. Tricyclic antidepressants are a potential cause of constipation. The possibility of sexual or rectal abuse should be explored. On physical examination, growth and weight-gain are important screens for medical causes of encopresis. Measurement of umbilical girth is a useful indicator of the degree of abdominal distention, especially for following response to fecal evacuation treatment. Hirschsprung’s disease is often included in the differential diagnosis of constipation, but a key clinical feature of Hirschsprung’s disease is the absence of encopresis.
Management
Prevention involves effective toilet training and treatment of constipation before it becomes chronic (Kiddoo et al., 2006). The success of encopresis treatment depends heavily on the understanding and cooperation of the patient’s family. The greatest success has been demonstrated when behavioral interventions are combined with aggressive laxative therapy (Brazzelli and Griffiths 2006). Biofeedback does not appear to add additional benefit. Treatment typically includes disimpaction with a series of enemas, followed by adequate laxatives and fiber supplements to produce at least one painless soft stool each day. Once the child establishes a regular bowel pattern of one to three stools per day without soiling episodes, the laxative dose is gradually decreased.
KEY TREATMENT
Enuresis is repeated voiding into the bed or clothing after a person has reached an age at which continence is expected. Enuresis is most frequently nocturnal (occurring at night) but can be diurnal (occurring during the day) or both. DSM-IV-TR defines the age at which continence is expected as 5 years, but as many as 15% to 20% of 5-year-old children have nocturnal enuresis. The spontaneous cure rate is 15% per year of age, leading to a prevalence of 5% to 10% in 10-year-olds and 1% to 2% in 18-year-olds. This prevalence indicates that nocturnal enuresis is second only to allergic disorders as the most common chronic ailment in childhood. Enuresis may be primary (child has never established urinary continence) or secondary (child becomes incontinent after an initial period of continence.
The etiology of enuresis is multifactorial, with a definite genetic component. When neither parent has a history of bedwetting, the incidence in their children is 15%. The incidence increases to 40% when one parent has a positive history and to 75% when both parents have a bedwetting history.
The pathophysiologic factors that lead to nocturnal enuresis are (1) overproduction of urine through the night, (2) abnormally small bladder volume, and/or (3) failure of arousal when the bladder is full. In regard to urine overproduction, there is evidence children with nocturnal enuresis have lower levels of nighttime antidiuretic hormone (ADH) than nonenuretic children. This phenomenon probably plays an important role in childhood enuresis but has not been demonstrated to be present in enuretic adolescents. Measured bladder capacity in those with nocturnal enuresis is usually normal. However, detrusor overactivity during sleep has been observed in many enuretic patients, suggesting that functionally reduced bladder capacity during sleep may play a role in as many as one third of children with nocturnal enuresis. Also, enuretic children are more difficult to arouse from sleep than nonenuretic children, as demonstrated by parent survey and sleep laboratory testing (Hjalmas, 1998).
Patients can be categorized as having uncomplicated nocturnal enuresis or complicated enuresis based on the initial history, physical examination, and urinalysis and culture. Children with uncomplicated enuresis have primary nocturnal enuresis but are otherwise asymptomatic and have negative physical exam and urine studies. Treatment can be initiated in these children without further workup. Complicated enuresis is any case that does not meet these criteria. With a greater possibility of a significant psychosocial problem or medical abnormality, these children merit more extensive evaluation based on the initial assessment findings.
Primary nocturnal enuresis is not usually caused by psychological factors. However, a history of enuresis that is solely diurnal suggests the possibility of significant psychosocial pathology. This risk should also be considered in patients with secondary nocturnal enuresis (i.e., child becomes incontinent at night after initially establishing continence). Stressors to consider in these patients include serious parent-child or teacher-child interaction problems, attention-getting behavior after a family system change (e.g., new sibling), and physical or sexual abuse.
Combined nocturnal and diurnal enuresis may be a symptom of a urinary tract infection (UTI). Mild urinary urgency and frequency of up to seven voids during the day are common in 7-year-olds (Hjalmas, 1998). However, significant daytime symptoms of urinary frequency and urgency even without incontinence, when combined with nocturnal enuresis, should lead to consideration of mechanical urinary problems such as posterior urethral valves. Also, if bowel incontinence accompanies the urinary incontinence, psychosocial pathology and neurologic abnormalities should be considered.
The physical examination should include specific attention to the abdomen, genitals, lower spine and neurologic function, and developmental and psychological appropriateness. The urinalysis and urine culture screen for metabolic diseases and UTI. Additional tests are reserved for patients with complicated enuresis, looking for specific secondary causes, and for patients with apparently uncomplicated nocturnal enuresis who fail initial treatment.
Because of the high prevalence and high spontaneous resolution rate, treatment of enuresis is not encouraged until the child is at least 6 years old. Successful treatment can normalize the low self-esteem that is a common consequence of enuresis (Hagglof et al., 1998). Particularly in patients with diurnal enuresis, however, psychosocial issues may need to be addressed before attempting treatment aimed at the enuresis alone.
A critical factor in successful treatment of enuresis is patient and family motivation. General recommendations for nocturnal enuresis are to (1) limit evening fluid intake, (2) establish a consistent bedtime routine that includes relaxed voiding, (3) avoid sleep deprivation, (4) focus on rewards for dry nights, (5) avoid punishment for wet nights, (6) make the child responsible for cleaning up clothing and bedding in age-appropriate manner and in a matter-of-fact, nonpunitive way, and (7) if the child is aroused to void after already asleep, make sure the child awakens fully to urinate.
Treatments for nocturnal enuresis target the individual potential etiologies: inadequate ADH secretion, detrusor overactivity, and high arousal threshold. Unfortunately, there are no routine clinical tests to differentiate these causes, so treatment choices must be made based on other criteria. That treatment lacks specificity in this way may account for a substantial proportion of treatment failures.
The three most common treatments for nocturnal enuresis are electronic enuresis alarms, desmopressin (DDAVP), and imipramine. All three approaches were found effective in a systematic review, with advantages and disadvantages for each (Glazener et al., 2009). Enuresis alarms work as a conditioning mechanism to facilitate arousal. A sensor is placed in the child’s underpants and connected to an alarm attached to the bed clothing. The sensor can detect a very small volume of urine, such that the alarm sounds before the child completes voiding. The aroused child can finish voiding in the toilet and change any wet linens or clothes. The alarms are more efficient treatment than medications but put greater demands on the child and family. Enuresis alarms are inexpensive (<$100) and widely available but may not be reimbursed by insurance carriers.
Desmopressin is a synthetic analog of arginine vasopressin, a natural antidiuretic hormone. It works by reducing overnight urine output. It is available as an oral tablet or a nasal spray. Desmopressin is expensive but is often covered by third-party payers. It is immediately effective but has a high relapse rate after discontinuation. The relapse rate can be minimized by rapid titration until dryness in 1 to 3 days, followed by maintenance therapy for at least 4 to 6 weeks, then very slow, stepwise dose reduction. Side effects are uncommon and generally mild. The risk of the rare but most serious potential side effect, seizures from hyponatremia, can be minimized by restricting evening fluid intake, as is recommended for enuresis in general.
Tricyclic antidepressants (TCAs), particularly imipramine, have been used for many years to treat enuresis. The usual dose of imipramine is 1 to 2 mg/kg at bedtime. It is usually continued for 6 to 8 weeks before tapering, and a second course may be given for relapses. Although inexpensive and effective, imipramine has a serious side effect profile, including potential cardiac arrhythmias and high toxicity in accidental overdose. Therefore, imipramine is generally not first-line treatment for enuresis.
With any of these management options, follow-up is important to improve compliance. Other forms of treatment, including bladder-training exercises to increase functional bladder capacity and anticholinergic medications to relax the bladder’s smooth muscle, have inadequate evidence of effectiveness to be recommended. Combination treatment with multiple modalities aimed at different etiologies (enuresis alarm plus desmopressin) has been suggested, particularly for refractory cases, but information on its effectiveness is limited. Children whose enuresis is accompanied by encopresis should have the encopresis addressed first. This is because the enuresis may resolve spontaneously once the pelvic mass of retained stool is evacuated, allowing the bladder to expand.
KEY TREATMENT
eBox 24-1 DSM-IV-TR Diagnostic Criteria for Oppositional Defiant Disorder
From American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text revision (DSM-IV-TR). Washington, DC, APA, 2000.
eBox 24-2 DSM-IV-TR Diagnostic Criteria for Conduct Disorder
From American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed, text revision (DSM-IV-TR). Washington, DC, APA, 2000.




