, Antonio Cesarani2 and Guido Brugnoni3
(1)
“Don Carlo Gnocchi” Foundation, Milano, Italy
(2)
UOC Audiologia Dip. Scienze Cliniche e Comunità, Università degli Studi di Milano, Milano, Italy
(3)
Istituto Auxologico Italiano, Milano, Italy
Abstract
Autonomic vertigo (AV) was described in 2003 by Pappas who showed a subgroup of patients with spontaneous vertigo who also demonstrated symptoms and findings consistent with poor autonomic regulation. Patients affected with AV describe symptoms that, in some cases, failed to improve or worsened with prior treatment of low-sodium diet or diuretics. Autonomic symptoms include palpitations, chronic fatigue, cold extremities and previous fainting. The key lesion of AV is dysregulation of autonomic vestibular responses. Pappas proposed as management of AV fluid loading, dietary changes, exercise and patient education. Rehab is aimed to improve postural control and to re-coordinate visuo-vestibular balance control with respiration.
In 2003 Pappas [1] showed a subgroup of patients with spontaneous vertigo who also demonstrated symptoms and findings consistent with poor autonomic regulation, that is to say, vestibular symptomatology can occur in relation to autonomic dysfunction. He defined this clinical entity as autonomic vertigo (AV).
Patients affected with AV describe symptoms consistent with spontaneous, rotational vertigo or postural vertigo and distinct lightheadedness. In some cases, vertigo failed to improve or worsened with prior treatment of low-sodium diet or diuretics.
Autonomic symptoms include palpitations, chronic fatigue, cold extremities and previous fainting. A history of mitral valve prolapse is frequent.
More recently Kim and Lee [2] showed that in patients with benign paroxysmal positional vertigo (BPPV), residual dizziness after successful treatment may be associated with sympathoneural autonomic dysfunction.
The key lesion of AV is dysregulation of autonomic vestibular responses. Although the neural signals generated from the hair cells of the otolith organs and semicircular canals are important in the maintenance of equilibrium and orientation, they influence also autonomic control, and thus, the third group of vestibular reflexes are the vestibulosympathetic or vestibulo-autonomic reflexes (VAR), provided by the labyrinth, through vestibular nuclei, besides the vestibulo-ocular (VOR) and the vestibulospinal (VSR) reflexes [3, 4].
Evidence suggests that the vestibular system plays a role in postural-related adjustments in blood pressure. Much like equilibrium, blood pressure regulation involves multiple feedback systems. The most recognized feedback system for blood pressure regulation is the baroreflex that senses mechanical changes in the blood vessels of the aortic arch and carotid bodies. However, Carter and Ray [5] provided direct evidence that the vestibulosympathetic reflex is a robust vascular reflex in humans and that the vestibular system is important in postural blood pressure regulation. Aging, through aging processes involving hair cells, attenuates the vestibulosympathetic reflex in humans and, in this way, it may contribute to the increased prevalence of orthostatic hypotension with age [6].
The vestibular autonomic reflexes influence also muscle sympathetic nerve activity (MSNA) which responses are specific to activation of the otolith organs and not the semicircular canals [7]. Sauder et al. [8] showed that the sensitivity of the vestibulosympathetic reflex is greater in the upright compared with the prone position supporting and further expanding the concept that the vestibulosympathetic reflex is a robust autonomic reflex.
Yates [9] showed that considerable evidence exists to suggest that both sympathetic and respiratory outflow from the central nervous system are influenced by the vestibular system and otolith organs that respond to pitch rotations seem to play a predominant role in producing vestibulosympathetic and vestibulo-respiratory responses.
Carter et al. [10] showed the additive neural interaction between mental stress and the vestibulosympathetic reflex: this interaction may induce post-traumatic stress disorders with vertigo and dizziness [11].
The autonomic nervous system, the hormonal systems and the postural control are strictly interconnected as assessed, for example, in adolescent idiopathic scoliosis in which the pathogenesis of developmental disharmony between somatic and autonomic nervous systems is postulated [12]. In fact, normal mechanisms involved in trunk growth, acquired in evolution and unique to humans, are driven hormonally and supplemented by the sympathetic nervous system acting symmetrically. Hormonal abnormalities, e.g. insulin resistance and hyperinsulinemia, are frequently observed in AV patients.
Pappas proposed as management of AV fluid loading, dietary changes, exercise and patient education.
Rehab is aimed to improve postural control and to re-coordinate visuo-vestibular balance control with respiration.
14.1 Exercises in the Gymnasium
14.1.1 First Week
1.
2.
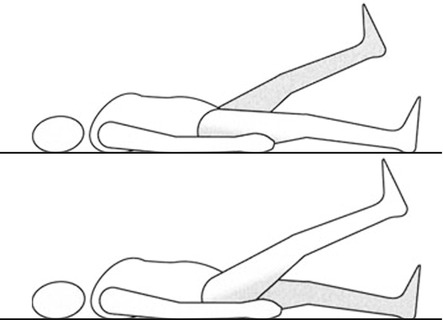
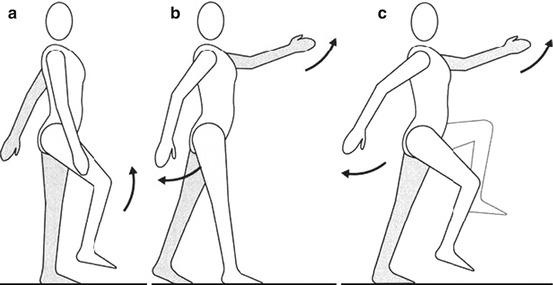
The patient extends the left arm over her/his head and simultaneously she/he moves the flexed right leg to the chest, with the help of her/his hands. She/he maintains this position for 10 s and then repeats with the opposite arm and leg (Fig. 14.2).
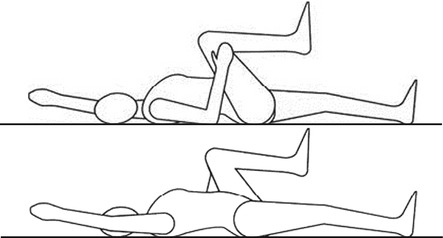
Fig. 14.2
Flexion of the knee with simultaneous extension of the opposite arm (Originally published in Cesarani and Alpini [14] published by Springer © 1999)
3.
The patient holds her/his left leg against the chest with the knee flexed, maintaining this position for 10 s and then repeats the exercise with the right leg. She/he then holds both knees against her/his chest (Fig. 14.3).
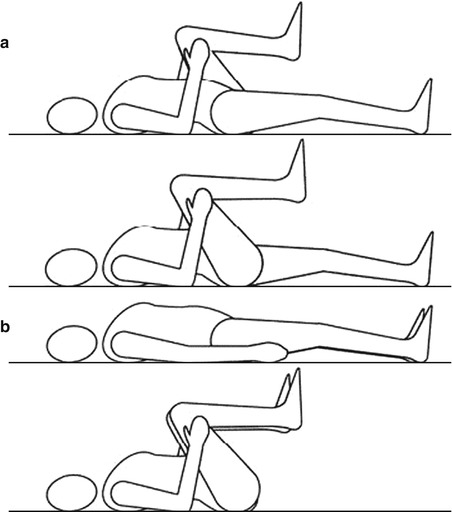
Fig. 14.3
(a, b) Exercises of the knees for the pelvis (Originally published in Cesarani and Alpini [14] published by Springer © 1999)
4.
5.
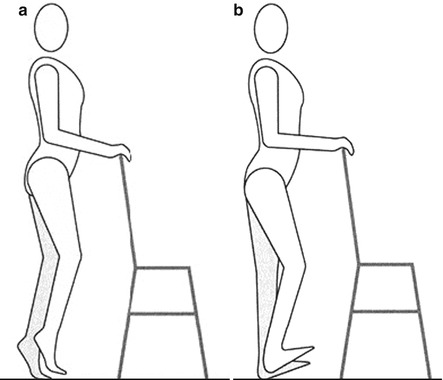
6.
The patient, with her/his hands on a chair, lifts her-/himself on her/his heels, maintaining this position for 30 s (Fig. 14.5b).
7.
10.
Standing on a balance board:
(a)
The patient oscillates to and fro, maintaining equilibrium with the arms.
(b)
The patient oscillates from side to side, maintaining equilibrium with the arms.
14.1.2 Second Week
1.
Get Clinical Tree app for offline access

The patient stands quietly in an upright position standing on tiptoes and fixating a target on a mirror. In this case, she/he receives from two planes of fixation: the target and her/his image. She/he needs to be able to extract the correct fixation information from visual inputs (Fig. 14.7a).
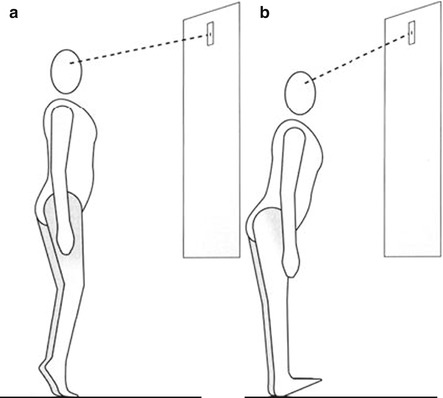
Fig. 14.7




Exercises on tiptoes (a) and heels (b) fixating a target on a mirror (Originally published in Cesarani and Alpini [14] published by Springer © 1999)
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree