Athletic Pubalgia and Adductor Injuries
Kostas Economopoulos
Anikar Chhabra
DEFINITION
Although the term sports hernia is commonly used in the media, athletic pubalgia is a more appropriate term to describe the constellation of injuries causing chronic groin pain in athletes.
Diagnosis of the cause of groin pain is difficult due to the complex anatomy of the groin and the fact that two or more injuries may coexist.
Intra-abdominal pathology, genitourinary abnormalities, referred lumbosacral pain, and hip joint disorders must first be excluded.
Adductor strains are the most common cause of groin pain in athletes.
The adductors are usually strained during eccentric contraction of the muscles. The injury often occurs at the myotendinous junction, but the strain also can occur in the tendon itself or its bony insertion.
Other muscles in and around the groin region also can be strained, including the rectus femoris, the sartorius, abdominal muscles, and the conjoint tendon.
Sports hernia is a condition of chronic groin pain that is caused by a tear in the inguinal floor without a clinically obvious hernia.7,11
Sports hernias result in an occult injury that usually is not identified by most examiners. However, with increasing experience, the examiner can feel an abnormal inguinal floor and appreciate abnormal tenderness inside the external ring.
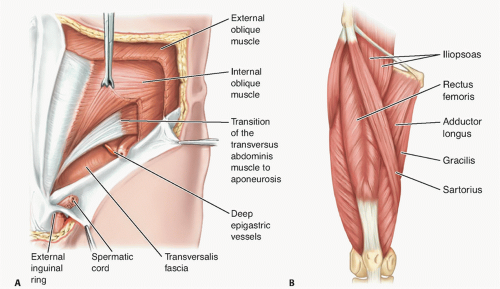
FIG 1 • Anatomy of the abdominal (A) and groin (B) musculature.
In contrast, indirect and direct hernias involve easily palpable defects in the inguinal canal or through the anterior abdominal musculature, respectively.
Duration of symptoms typically is months, and pain is resistant to conservative measures.
Osteitis pubis is characterized by symphysis pain and joint disruption and occurs commonly in distance runners and soccer players.
It may be difficult to distinguish from adductor strains, and the two conditions may coincide.
Stress fractures are rare injuries that result from repetitive cyclic loading of the bone.
The pubic rami are the most common location for stress fractures in the pelvis. These fractures are most common in long-distance runners.
ANATOMY
The anatomy in and around the groin is complex (FIG 1), and a thorough understanding of it is crucial in diagnosing the various groin injuries.
In terms of athletic pubalgia, the pelvis is considered to contain two joints: the commonly known ball-and-socket of
the hip joint and the second, less well known “pubic bone joint.”
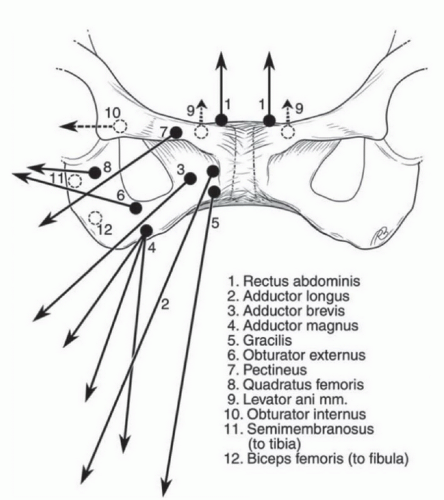
FIG 2 • Pubic bone joint. The pubic bone joint is made up of the anterior bone structures of the pelvis and all of the soft tissue attachments to the pubic bones. This diagram shows the many structures which attach to the anterior pelvis and the forces that are placed on the pubic bone joint. (Reprinted with permission from Meyers WC, Greenleaf R, Saad A. Anatomic basis for evaluation of abdominal and groin pain in athletes. Oper Tech Sports Med 2005;13:55-61.)
The pubic bone joint consists of a large, complex rotational joint that involves both pubic bones and all the soft tissue attachments on either side of the pubis (FIG 2).
The pubic symphysis is the center point of the pubic bone joint and is the site of numerous musculotendinous attachments that act to dynamically stabilize the position of the anterior pelvis.
The abdominal muscles attaching to the pubic symphysis consist of the external and internal oblique muscles, transversus abdominis, and rectus abdominis. The thigh adductors attaching to the pelvis include the pectineus, gracilis, adductor longus, brevis, and magnus.
The posterior inguinal wall consists primarily of the transversalis fascia, along with the conjoint tendon, made up of the internal abdominal oblique and transversus abdominis aponeuroses.7
The conjoint tendon inserts onto the pubic tubercle and along the iliopubic tract.
PATHOGENESIS
The most robust and important muscles for maintaining stability of the anterior pelvis are the rectus abdominis and the adductor longus muscles.
These muscle groups pull the pelvis with opposite vectors and function as antagonists to one another during flexion, extension, and rotation of the pelvis (FIG 3).
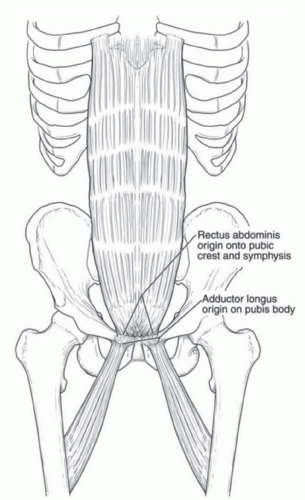
FIG 3 • Abdominis rectus and adductor attachments. The most important muscles in maintaining pelvis stability are the abdominis rectus and adductor muscles. These structures have a common attachment site on the anterior pubis and pull the pelvis in opposite directions. (Reprinted with permission from Meyers WC, Greenleaf R, Saad A. Anatomic basis for evaluation of abdominal and groin pain in athletes. Oper Tech Sports Med 2007;15:165-177.)
A tremendous amount of torque is created at the level of the pelvis in athletes participating in sports requiring twisting and cutting. The cutting and twisting activities require the use of the abdominal and pelvic muscles, which creates significant force through the pelvis and stress on the tendinous insertions.
Overuse injuries due to repetitive hip hyperextension and truncal rotational movements lead to wear and tear of the tendon insertions culminating in partial or full tearing of these structures. When one muscle weakens or its associated tendon torn, the result is an unequal distribution of pelvic forces and overpulling of one of the muscles leading to more anterior or posterior pelvic tilt, depending on which muscle or tendon is injured.
NATURAL HISTORY
A majority of acute adductor strains will improve with appropriate conservative treatment over a course of 2 to 6 weeks. However, if not properly rehabilitated, an adductor injury may progress to chronic strains or tendinopathy.
Recovery from athletic pubalgia varies greatly from athlete to athlete. Although many athletes will get improvement with rest and conservative treatment, recurrent symptoms are common after returning to play. A small subset of patients will improve with nonoperative treatment; however, most patients who have been accurately diagnosed with athletic pubalgia will eventually require surgical repair.7,13 A hallmark of sports hernias is that patients have less pain when they are inactive and more pain when active.
Osteitis pubis is self-limited but may take, on average, about 9 months to heal.5
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient history is the most important aspect of the evaluation of athletic pubalgia.
The patient must be asked for duration of symptoms, any inciting events, relieving and exacerbating factors, and timing of pain.
A thorough hip examination must be performed to rule out intra-articular hip sources of pain such as labral tears and femoroacetabular impingement (FAI).
Flexion, adduction, and internal rotation of the hip are used to identify anterior FAI. The FABER test (flexion, abduction, and external rotation of the hip) is used to identify posterior impingement.
Decreased hip internal rotation is common in patients with cam-lesion FAI. Internal rotation of less than 25 degrees is considered abnormal.
Hip flexion against resistance: tests the strength of the iliopsoas and may detect a strain or tear of this muscle.
Groin examination:
Palpation of the insertion of the rectus and origin of the adductors can identify partial tears, inflammation, or injury to these tendons.
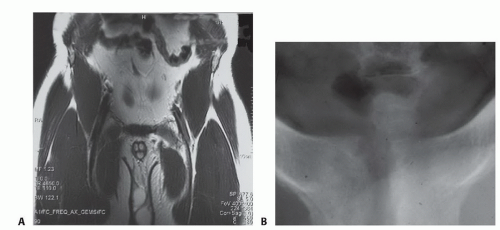
FIG 4 • A. MRI of an adductor tear in a hockey player. There is increased signal at the origin of the adductor tendon near the pubis. B. Characteristic radiograph of osteitis pubis. Notice the bone resorption, widening of the pubic symphysis, and irregular contour of articular surfaces.
Palpation of insertion of conjoint tendon: Tenderness may increase, and a bulge may be felt by having the patient perform a Valsalva maneuver.
Straight-leg raise: In patients with radicular low back pain, this will reproduce the pain they are having.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



