I. GENERAL GUIDELINES
A. For any injection, consider infiltrating the subcutaneous skin of the entry site. It will improve the patient’s comfort, and it will allow one to make several attempts without extra discomfort for the patient. Using an ethyl-chloride-based spray is a reasonable alternative to “freeze” the skin in the area of the injection.
B. When using corticosteroids, be aware of the possibility of subcutaneous atrophy or skin color changes if the medication is left subcutaneously.
C. In an obese patient, be prepared to use spinal needles.
D. Use larger gauge needles with large syringes (20 cc and above) if an aspiration of a joint is going to be performed as blood or pus presents a thicker texture than synovial fluid.
When trying to rule out a septic joint, avoid having the entry site over the area of cellulitis as this will contaminate the joint and eventually the sample sent to the lab.
II. THE SHOULDER JOINT (i.e., the glenohumeral joint) may be entered either anteriorly or posteriorly as depicted in Fig. 30-1. When using the anterior approach, palpate the medial aspect of the humeral head and enter just medial to this. In our experience, more physicians now prefer a posterior approach. A posterior aspiration or infiltration of the shoulder is performed with an entry site located approximately 2 cm distal and 1 cm medial to the posterior corner of the acromion (Fig. 30-1B). At this level, the “soft spot” of the shoulder can be felt. The needle will be placed perpendicular to the posterior chest wall and aiming for the coracoid process, which is felt over the anterior aspect of the shoulder with the opposite hand. A “pop” will be felt when the capsule is penetrated with a medium-sized needle. Slight rotation of the arm may be used to confirm if the needle tip is over the glenoid rim versus the humeral head and the need for any relocation of the needle.
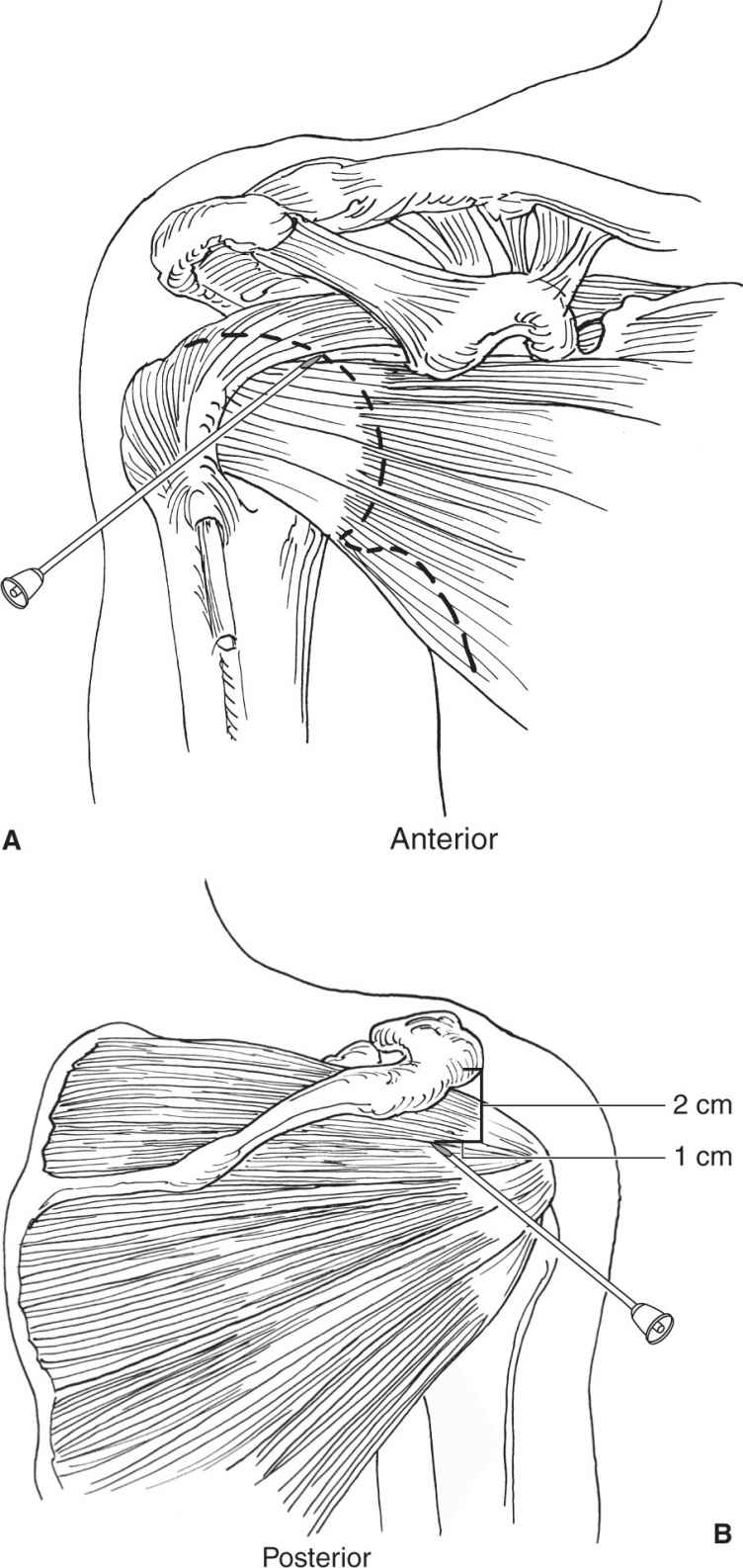
Figure 30-1. Shoulder joint and subacromial space.
Using the same entry site and with an angle of approximately 30° cephalad, the subacromial space can be reached. Sometimes if the needle is angled too superiorly, or in an obese patient, the needle will hit the posterior margin of the acromion and it will have to be “walked” into the subacromial space.
III. THE ELBOW JOINT (Fig. 30-2). The elbow will present a semi-flexed position secondary to the pain and increased intraarticular fluid. The entry site will be located at the center of the triangle formed by the lateral epicondyle, the radial head, and the most lateral corner of the olecranon. At this level, the “soft spot” of the elbow joint is felt and the elbow joint can be easily reached. A second approach can be done immediately proximal to the superior margin of the olecranon and centered over the middle third of the olecranon through a transtendinous approach for the triceps tendon. This would provide full access to the olecranon fossa.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


