CHAPTER 23 Arthroscopically Assisted Treatment of Intraosseous Ganglions of the Lunate
Introduction
Intraosseous ganglia of the carpal bones are an infrequent cause of chronic wrist pain. The pathogenesis remains obscure.1,2 Bone scans and computerized tomography (CT) are used to distinguish these radiolucent carpal lesions from other pathologies, in particular degenerative cysts and osteoid osteomas.1 Magnetic resonance imaging (MRI) will demonstrate the bony extent of the lesion and may help to delineate the presence of an extraosseous extension of the ganglion.3
Persistence and severity of symptoms rather than radiological findings determine the need for further management.4 Curettage and bone grafting have been performed for patients with constant symptoms that have severely restricted their occupational or recreational activities.1–6 Clinically, the patients improve. However in up to 40% symptoms persist that affect function.1,2 The authors have published a minimally invasive technique of lunate ganglion grafting with the aim of reducing the morbidity that has been seen with open techniques.7
Pathology
Theories of pathogenesis of ganglia have included synovial herniation, neoplasia, metaplasia of mesenchymal precursor cells, proliferation of synovial rest cells, and traumatic mucoid degeneration of connective tissue.1,2 The shear stresses concentrated at the scapholunate ligament insertion may predispose some individuals to developing the precursor cells that form the intraosseous ganglion.8 Rather than proliferating dorsally from the scapholunate ligament, the cells head into the lunate itself.
Intraosseous ganglia are pathologically identical to the soft-tissue variety, with a thin wall of compressed collagen and fibroblasts containing a clear viscous fluid that has a high concentration of hyaluronic acid.1–4,6,8–11 There is no endothelial or synovial lining. A thin sclerotic margin of bone often surrounds the ganglion. Some authors have suggested that this represents an attempt by the host bone to repair the defect within the lunate.2 Bone scans invariably show increased uptake localized to the involved carpal bone. The advantages of arthroscopic surgery versus open techniques to treat lunate ganglion cysts include a lower morbidity and less risk of damaging the scapholunate ligament.
Indications
The patient presents with persistent dorsal wrist pain and swelling in the perilunate region that is exacerbated by activity and reduced grip strength. The decision to operate is based on the persistence and severity of the symptoms rather than on the outcome of the investigations, which help to localize the pathology. Preoperative symptoms often interfere with function at work or during recreation.1,2,4
Patients were not considered for surgery unless they had been symptomatic for at least six months and had failed a trial of activity, NSAIDs, and splints. Assessment included clinical examination for local tenderness and carpal stability. Radiographs usually revealed an eccentrically placed radiolucent lesion with a thin sclerotic margin contained within and not expanding the lunate (Figure 23.1).

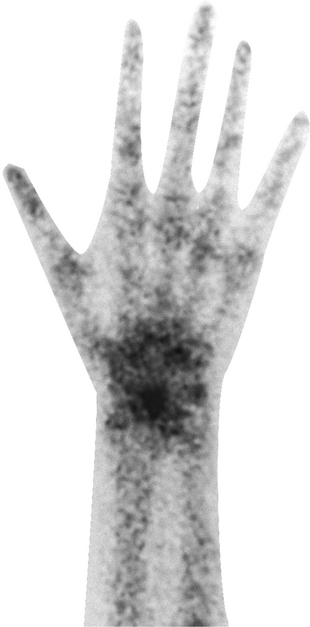
All patients had a preoperative technetium 99 radionuclide bone scan demonstrating focal increased uptake within the lunate and no other site within the wrist (Figure 23.2). This investigation helped to confirm that the patients’ symptoms were related to the intraosseous ganglion prior to any intervention. Patients who had a negative bone scan were not offered surgical treatment.
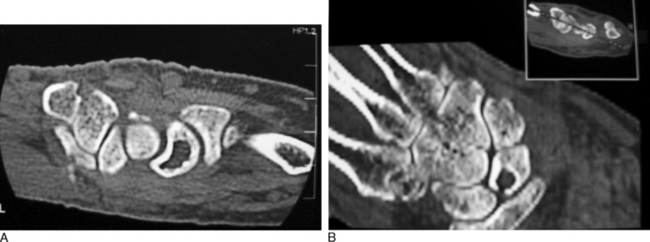
CT scans were used to define the location and extent of the lesion, which aided surgical planning. Localization of the cyst is particularly important with this technique, as the cyst may be volar or dorsal. Figure 23.3 shows a typical coronal CT scan in which the ganglion located close to the scapholunate ligament can be seen to perforate the cortex of the lunate at the site of attachment of the ligament. It is a common radiological finding, and confirms its origin as a ganglion from the scapholunate ligament. Some surgeons have previously interpreted this as a fracture.
Contraindications
Lesions with more sinister pathology of lesion need to be excluded. These are rare and can be differentiated with imaging. Other common pathological conditions that affect the lunate include Kienbock’s diseases and avascular necrosis, which produces sclerosis and often collapse of the proximal convexity of the lunate 22 (Figure 23.4a). Ulnar carpal impaction is also common, but this affects only the ulnar side of the lunate and is often associated with a kissing lesion of the ulnar head (Figure 23.4b). Bone islands (Figure 23.4c), osteoid osteoma, and other lesions are rare. CT scans can help differentiate these lesions.
< div class='tao-gold-member'>

Related posts:
 Arthroscopy of the Distal Radioulnar Joint
Arthroscopy of the Distal Radioulnar Joint
 Arthroscopic Plication of Lunotriquetral Ligament Tears
Arthroscopic Plication of Lunotriquetral Ligament Tears
 Arthroscopic Treatment of Scapholunate Ligament Tears
Arthroscopic Treatment of Scapholunate Ligament Tears
 Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
 Wrist Arthroscopy Portals
Wrist Arthroscopy Portals
 Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


