CHAPTER 19 Arthroscopic Wrist Capsulotomy
Introduction
Wrist contractures can occur following any type of wrist injury, but are most prevalent following distal radius fractures. Ganglion excision, carpal dislocation or fracture, previous wrist surgery, reflex sympathetic dystrophy, and prolonged immobilization may all lead to a loss of wrist motion. Watson has previously described a release of the volar and dorsal wrist capsule through open capsulotomies.1 A similar approach has been described for the distal radioulnar joint.2 Arthroscopic release of wrist contractures has been reported by a number of authors, with encouraging results.3–5
Indications
A biomechanical study performed by Palmer et al. defined functional wrist motion as being flexion of 5 degrees, extension of 30 degrees, radial deviation of 15 degrees, and ulnar deviation of 10 degrees.6 Patients lacking a functional arc of wrist motion who have failed a trial of dynamic/static progressive splinting are candidates for this procedure. Volar capsulotomies are less risky and are indicated to regain wrist extension. Dorsal capsulotomies are necessary to regain wrist flexion but they may require use of a volar arthroscopy portal and are technically more difficult.
Contraindications
Contraindications in this case include all of those general to wrist arthroscopy, including active infection, large capsular tears (which can lead to extravasation of irrigation fluid), bleeding disorders, neurovascular compromise, marked swelling (which distorts the anatomy), inadequate or marginal soft–tissue coverage of the wrist, and the inability to withstand anesthesia. Division of the radioscaphocapitate (RSC), long radiolunate (LRL), and short radiolunate (SRL) ligaments should be performed with caution in patients who are at risk for ulnar translocation (such as those patients with rheumatoid arthritis and those who have undergone previous radial styloidectomies).7,8 A frank carpal volar or dorsal carpal instability pattern is another contraindication because release of the volar and/or dorsal extrinsic ligaments would likely exacerbate this condition.
Surgical Technique
Volar Capsulotomy
The procedure is done under tourniquet control. A 3−/,4 portal and 4−/,5 portal are established as described in Chapter 1. Inflow through the scope with outflow through a cannula in the 6–R portal is standard, although it may be necessary to switch in cases where adhesions block the flow. The radiocarpal joint space is identified with a 22–gauge needle and the joint is inflated with saline. A contracted joint may accept only a small amount of fluid.
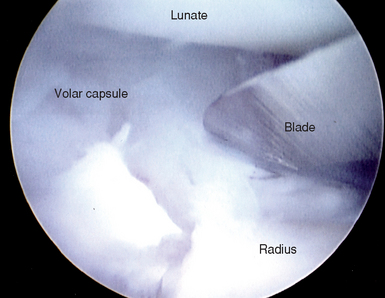
A suction punch and full–radius resector are used to clear adhesions off the volar capsule until the RSC, LRL, radioscapholunate ligament (RSL), and SRL are well defined. While viewing through the 3−/,4 portal, an arthroscopic knife is introduced through a cannula placed in the 4−/,5 portal (Figure 19.1). The cannula is necessary in order to protect the extensor tendons from inadvertent laceration during insertion and removal of the knife. The tip of the blade should be visualized at all times to prevent inadvertent perforation of the capsule or chondral damage. The RSC ligament is gently sectioned until the volar capsular fat and/or the flexor carpi radialis tendon is seen. Anatomical and MRI studies by Verhellen and Bain established that the radial artery was closest to the joint capsule at an average distance of 5.2 mm, the median nerve 6.9 mm, and the ulnar nerve 6.7 mm.5
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


