Arthroscopic Treatment of Valgus Extension Overload
Jonathan H. Capelle
Larry D. Field
ANATOMY
The bony articulation of the elbow joint provides primary stability to varus and valgus force at angles of less than 20 degrees and greater than 120 degrees of flexion.
Soft tissues are the chief stabilizers between 20 and 120 degrees, where most athletic activity occurs.
The ulnar collateral ligament (UCL) is the primary restraint to valgus stress.
It is composed of the anterior band, the posterior band, and the transverse ligament.
The anterior band is further divided into anterior and posterior bundle, which perform reciprocal functions (FIG 1).
UCL insufficiency can be subtle, with ligament-sectioning studies showing a 3-degree difference when the anterior band of the UCL is cut.3
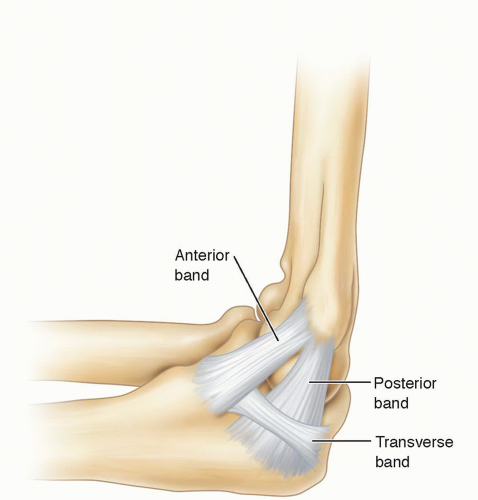 FIG 1 • The UCL is composed of three bands: anterior, posterior, and transverse. The anterior band is further subdivided into the anterior and posterior bundles. |
PATHOGENESIS
Valgus extension overload typically occurs in repetitive overhead athletes, most commonly with pitchers. The repetitive pitching motion imparts a large valgus force on the elbow. Resulting microtrauma and incomplete recovery can lead to attenuation of the UCL.
Failure of the UCL leads to abnormal valgus rotation of the elbow, affecting the mechanics of the highly constrained articulation of the posterior elbow joint.
This leads to bony impingement of the posteromedial olecranon and its corresponding fossa.
NATURAL HISTORY
Thus far, no studies have been performed documenting the natural history of the disease process.
It is postulated that chronic impingement and valgus extension overload can lead to posteromedial olecranon osteophyte formation that can cause ulnar nerve irritation and loss of elbow extension as well as posterior compartment elbow arthritis.
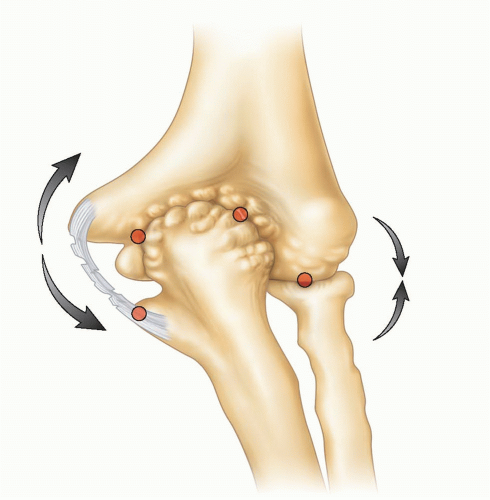 FIG 2 • Valgus extension overload. With UCL insufficiency, medial compartment distraction and lateral compartment compression ultimately lead to posteromedial olecranon impingement. |
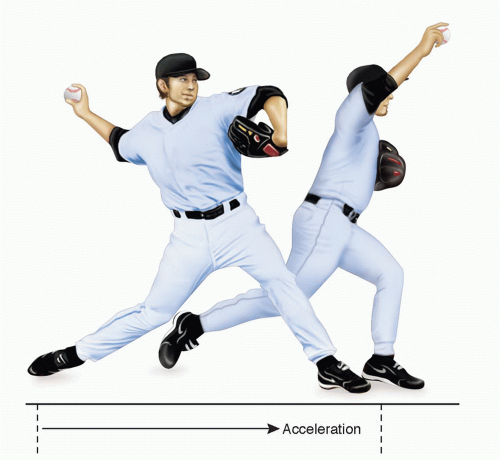 FIG 3 • The pitching athlete with valgus extension overload will often complain of pain during the acceleration and follow-through phases of throwing. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient typically complains of loss of extension with posterior or posteromedial elbow pain.
Pitchers will often report decrease in velocity and/or control as well as pain during late acceleration and early followthrough phases of the throwing motion (FIG 3).
Physical examination maneuvers relevant to valgus extension overload include the following:
Valgus extension overload test: This maneuver acts to simulate impingement occurring with the throwing motion and to reproduce the symptoms of posterior elbow pain.
Valgus stress test: Increased medial joint space opening, loss of end point, or pain elicited is significant for UCL insufficiency.
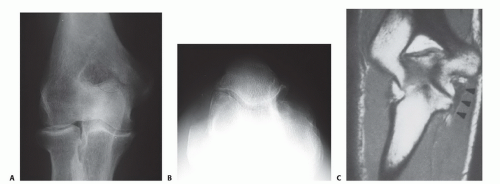
FIG 4 • Anteroposterior (A) and olecranon axial (B) radiographs showing spur formation along the posteromedial olecranon. C. Coronal section of MRI demonstrating injury to the UCL.
Milking maneuver: Maneuver eliciting pain, apprehension, or instability indicates UCL insufficiency.
Posterior olecranon impingement
Range of motion of elbow: may reveal loose bodies, chondromalacia, or osteophyte formation; flexion contracture may signify either osteophyte impingement or anterior capsular contracture.
Examination of the elbow should also evaluate for other causes of medial-sided elbow problems, such as isolated UCL insufficiency, ulnar neuropathy, medial epicondylitis, and flexor-pronator rupture.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs frequently reveal a posterior olecranon osteophyte on standard lateral or anteroposterior views (FIG 4A).
Some authors also advocate an olecranon axial view (FIG 4B).
Because radiographs cannot predict chondral lesions and soft tissue injuries and often underestimate loose body formation, magnetic resonance imaging (MRI) and computed tomography are frequently used.
MRI can also be important in investigating a potential UCL tear (FIG 4C).Related posts:
 Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Posterior Shoulder Instability
 Glenoid Bone Graft for Instability with Bone Loss
Glenoid Bone Graft for Instability with Bone Loss
 Athletic Pubalgia and Adductor Injuries
Athletic Pubalgia and Adductor Injuries
 Repair of Acute and Chronic Patella Tendon Tears
Repair of Acute and Chronic Patella Tendon Tears
 Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
 Modified Brostrom and Brostrom-Evans Procedures
Modified Brostrom and Brostrom-Evans Procedures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


