CHAPTER 8 Arthroscopic Treatment of Scapholunate Ligament Tears
Introduction
Scapholunate interosseous ligament (SLIL) injuries are one of the most common causes of mechanical wrist pain. Despite an increased knowledge of carpal injuries and improvements in radiologic evaluation, the diagnosis of an SLIL tear can be difficult or missed unless the evaluating physician has a high index of suspicion and an appropriate level of understanding of wrist anatomy and injury patterns. Usually a detailed history, physical examination, and a series of plain radiographs are sufficient to make a diagnosis of SLIL injury (Figure 8.1). Occasionally, advanced imaging (such as MRI with or without intra-articular contrast) can be helpful in establishing a diagnosis and evaluating the wrist for associated injuries.1–3 However, MRI usually detects large complete tears better than partial smaller tears, particularly if the tear configuration is oblique to the imaging plane or the tear is smaller than the distance between contiguous image slices.

After successful introduction in the knee and shoulder, arthroscopy gained popularity as one of the most useful modalities for diagnosing and treating a wide spectrum of wrist pathology.4,5 This procedure has become the gold standard for diagnosis of SLIL injuries.6–8 Arthroscopy is a minimally invasive procedure allowing direct observation of intrinsic and extrinsic carpal ligaments as well as articular cartilage integrity under static and dynamic conditions. Therefore, comprehensive and accurate diagnosis and treatment of all carpal injuries can be performed concurrently.
Because a delayed or missed diagnosis of an SLIL tear can lead to progressive carpal instability and predispose the patient to a predictable pattern of carpal arthritis called scapholunate advanced collapse (SLAC),9–11 we believe that wrist arthroscopy should be considered early during the evaluation and management of a patient with a suspected SLIL injury. However, it should be used selectively for patients with significant symptoms (a mechanism of injury consistent with SLIL injury) and in whom conservative treatment has failed or for whom acute operative management is indicated.
Anatomy of the Scapholunate Complex
The wrist is a complex structure comprised of multiple small-joint articulations with stability resulting from a complex linkage of intrinsic intercarpal ligaments and extrinsic capsular ligaments. The wrist can be thought of as 2 separate rows—with hand motion being the composite effect of motion among the radius, ulna, proximal carpal row (scaphoid, lunate, and triquetrum) and distal carpal row (scaphoid, trapezium, trapezoid, capitate, and hamate). Thus, the scaphoid is uniquely situated in both rows on an oblique axis to stabilize the carpus while still permitting coordinated relative motion between the two rows and the radius and ulna. The scaphoid is stabilized by many ligaments, including the SLIL, radioscaphocapitate, scaphotrapeziotrapezoid, scaphocapitate, and dorsal intercarpal ligament.12
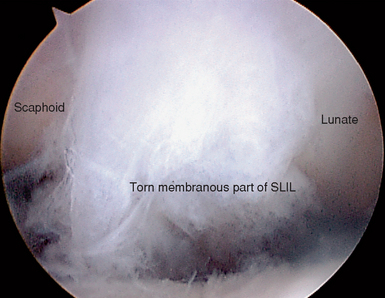
The SLIL is a C-shaped structure connecting the dorsal, proximal, and palmar surfaces between the scaphoid and the lunate—leaving the distal aspect of the joint bare of soft tissue and allowing the evaluation of scapholunate articular congruity, preservation, and instability. This midcarpal visualization is essential in assessing the degree of instability between the two bones and in grading the spectrum of partial to complete injury.13 The dorsal and palmar portions of the SLIL are true ligamentous structures.14 The proximal portion is a membranous structure composed mainly of fibrocartilaginous tissue.
In the absence of a tear, the transition between the dorsal and proximal portions is not readily visualized during arthroscopy. However, palpation of the SLIL with a probe permits differentiation between the thick taut dorsal ligament and the softer thin proximal portion. A partial SLIL tear may appear as a patulous convex outpouching rather than as a confluent (barely discernible) structure (Figure 8.2). Furthermore, the probe may uncover a complete disruption of the insertion of the SLIL—often from the lunate, which could not be perceived with observation alone. Partial tears may require palpation in the radiocarpal joint with a probe (to appreciate the laxity) and a thorough evaluation of the distal scapholunate joint articular surface congruity in the midcarpal joint to observe subtle incongruity or diastasis. A significant complete intrasubstance SLIL tear will be readily visualized in both the radiocarpal and midcarpal joints.
Biomechanical and Kinematics Considerations
The three different portions of the SLIL have different biomechanical properties. The dorsal portion of the SLIL has highest load at ultimate failure, followed by the palmar portion, and then the proximal portion.15 Serial sequential ligament sectioning studies in cadavers have found that the SLIL is the primary ligament scapholunate stabilizer.16–21 However, no significant dissociation between the scaphoid and the lunate is shown on static radiographs with an isolated complete SLIL disruption.16,22 This is explained by the presence of secondary stabilizers of the SL joint, which must be injured either acutely or chronically to demonstrate radiographic instability. Injury to the volar extrinsic (radiolunate, radioscaphocapitate),16,23 distal intrinsic (scaphotrapezial),16,24 or dorsal intercarpal ligament and the SLIL is needed to radiographically visualize pathologic carpal bone rotation.25
Changes in the radiocarpal, intercarpal, and midcarpal joint contact areas and loads in conjunction with the altered kinematics result in predictable SLAC arthritis. This begins with radial styloid beaking and radial styloid-scaphoid joint narrowing (stage 1), which then progresses proximally to alter the radial scaphoid facet proximal pole scaphoid articulation (stage 2) and then the midcarpal capitolunate joint (stage 3).9
Treatment Options
Several factors need to be considered to aid the clinical judgment indicating an arthroscopic procedure, not only to diagnose but to treat symptomatic scapholunate injuries (Figure 8.3). Acute repairable lesions have heretofore been treated with open suture repair or reattachment with bone anchors. Previous reports have sought to separate acute injuries from chronic by using an arbitrary and unproven 6 weeks as a cutoff, with the implied understanding that only acute injuries could be repaired. However, because the patient history is often unreliable as to the first subtle injury versus the most recent and now symptomatic injury dates alone should not indicate irreparable ligaments.
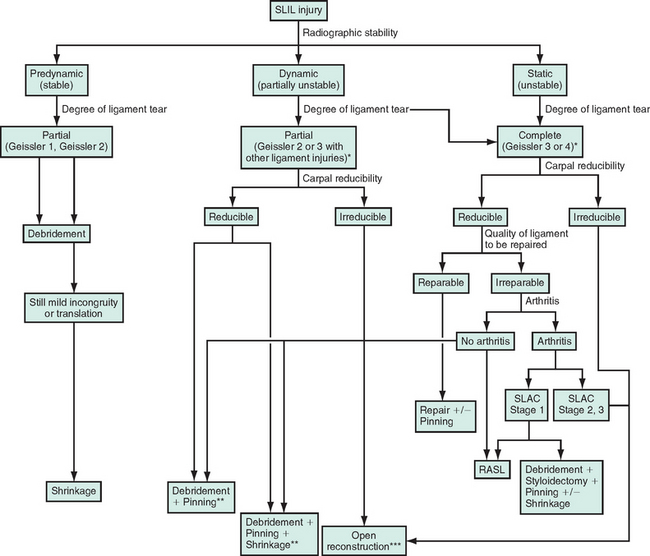
Stable wrists with symptomatic tears (pre-dynamic radiographic instability) are assumed after obtaining normal static and stress radiographs. Unstable wrists with tears demonstrable on grip films or cineradiography only (dynamic radiographic instability) have abnormal carpal alignment on stress radiographs (for example, pronated posterior-anterior grip) but normal alignment on unloaded routine radiographs. Unstable wrists with static instability on routine plain films (static radiographic instability) are the injuries that are obvious and thus not missed. However, these wrists may have advancing cartilage degeneration that is often underappreciated (especially at the capitolunate joint). The presence of significant polyarticular arthritis changes treatment options and often precludes reconstruction and indicates salvage procedures that usually fall outside the purview of arthroscopy (save for the master arthroscopist).
Arthroscopic assessment guides and rationalizes the potential for repair by confirming the degree of injury and the severity of instability.13 Arthroscopic treatment options include the following, either in isolation or in combination: ligament debridement, ligament thermal shrinkage, transarticular Kirschner wire fixation, and radial styloidectomy (Figure 8.3).
Complete repairable tears in the senior author’s (MPR) experience are best managed with open techniques. If the dorsal ligament has been avulsed from its attachment, it can and should be primarily repaired either with transosseous suture or suture anchor. Depending on the amount of associated soft-tissue injuries, this can be augmented with any of the numerous variations on dorsal capsulodesis.26–28
SLAC wrist evolution beyond the radial styloid and scaphoid wrist articulation often requires more extensive open surgical procedures. Complete irreparable tears in a young and active patient with a wide scapholunate diastasis and significant carpal mal-rotation should be considered for any procedure that can realign the carpus and preserve carpal kinematics so that the natural history of end-stage SLAC wrist can be forestalled. One such procedure used by the senior author since 1989 is the reduction and association of the scaphoid and lunate (RASL), creating an SLIL neoligament and protecting the repair with a transosseous SL headless bone screw.
Arthroscopic Debridement
Indications
Arthroscopic debridement alone is indicated for acute or chronic partial but stable tears of the volar or membranous portion of the ligament in a patient with mechanical symptoms (Figure 8.4). These patients usually have focal reproducible mechanical wrist pain over the dorsal scapholunate joint worsened by activity and normal X-rays. It is common to treat these patients conservatively for several months with splints and activity modification. Persistent symptoms often lead to an MRI, which rarely provides a definitive diagnosis and certainly does not illuminate the treatment options.
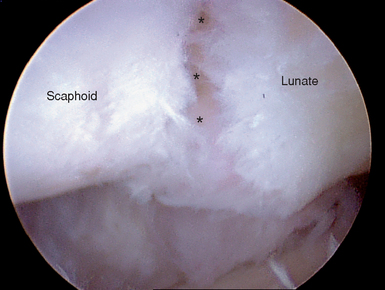
FIGURE 8.4 In the patient from Figures 8.1 and 8.2 the scapholunate joint (*) is visible after debridement of the membranous portion of the scapholunate ligament.
Contraindication to Debridement Alone
An absolute contraindication is a complete reparable tear or a more advanced Geissler instability pattern that was underappreciated in the preoperative evaluation. Static instability patterns with preexistent arthritis will not be helped save in a few selected cases of elderly patients with relatively low demand. A staged debridement and synovectomy can be offered with the full understanding that it may fail and necessitate a more comprehensive salvage procedure.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


