CHAPTER 11 Arthroscopic Treatment of Lunotriquetral Ligament Injuries
Mechanism of Injury
The wrist is an extremely complex joint.1 Its osseous and ligamentous anatomy as well as the normal carpal kinematics have been well studied.2–5 There are intrinsic ligaments that both insert and originate on the carpal bones, and extrinsic ligaments that insert on the carpal bones but originate on the wrist outside the carpus. The LTIL is the intrinsic interosseous ligament that stabilizes the lunate to the triquetrum (i.e., the LTJ). The LTJ is found along the ulnar portion of the proximal carpal row (PCR), which consists of the scaphoid, lunate, and triquetrum.
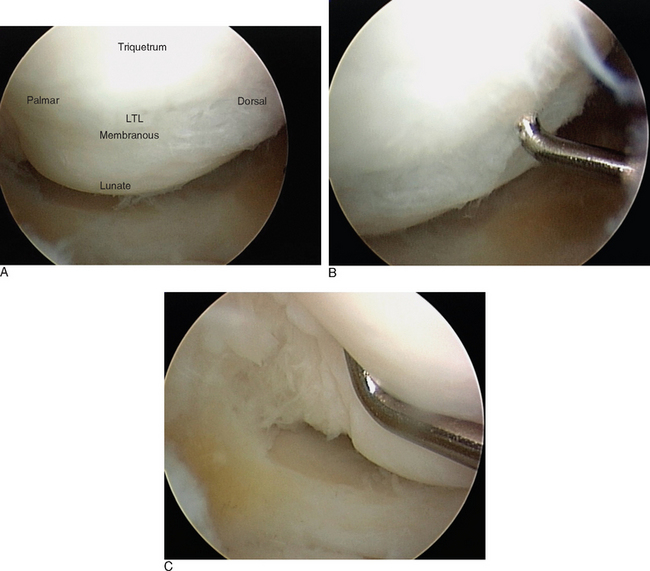
The PCR acts as an intercalated segment (IS), providing a mechanical linkage between the distal carpal row and the distal radius and ulna. There are three distinct regions of the LTIL (Figure 11.1). The dorsal and palmar portions are thickened and provide a strong, stable connection at the LTJ. The palmar portion of the LTIL is the thickest and strongest of the three regions, and is most important in the transmission of load and strain from the triquetrum to the lunate. The central, proximal portion of the LTIL consists of a fibrocartilaginous membrane that provides minimal joint stability.6
Carpal instability (CI) is the end result of a wrist ligamentous injury, which may occur from a variety of mechanisms. The failure of wrist ligaments (and the resultant carpal instability) causes pain (i.e., a symptomatic dysfunction), produces abnormal carpal kinetics (i.e., altered stress with the inability to bear functional loads), and abnormal joint kinematics (i.e., abnormal carpal motion).7 The degree of instability can vary from a subtle micro-movement due to ligament attenuation to gross carpal displacement with a wide intracarpal gap and abnormal carpal alignment.8–16
With an injury to the LTIL, the normal kinetics and kinematics of the wrist are disturbed.17,18 A spectrum of LTJ injuries can develop, ranging from a mild sprain with or without dynamic instability to a complete disruption with a secondary carpal instability dissociative (CID) pattern. This may culminate in a static altered carpal alignment, often referred to as volar intercalated segment instability (VISI). A static CI is characterized by a fixed dissociation between carpals that is clearly evident on imaging studies or during arthroscopy. A dynamic CI is characterized by normal routine radiographs, abnormal kinematics on stress imaging, or altered kinetics and kinematics viewed during arthroscopy.
The mechanism of LTIL tearing resulting in injury to the LTJ is somewhat controversial.19 Perilunate and reverse perilunate injury patterns caused by dorsally and/or palmarly applied forces, fractures of the distal radius or carpals, degenerative wear from ulnar abutment, prolonged repetitive stress, and inflammatory arthritis/synovitis have all been implicated.20,21 Furthermore, the presence of an ulnar positive variant at the DRUJ can facilitate attritional wear and tear of the LTIL.22–24
Most investigators believe that when the LTIL is injured subtle micro-motion instability begins, which results in wrist joint synovitis and subsequent chondromalacia.6 Some investigators would consider this early stage as a predynamic instability. Interestingly, damage to the intrinsic interosseous ligament alone is usually not sufficient to cause LTJ dissociation and a grossly unstable VISI. Additional tearing of the secondary constraints to the LTJ is necessary to produce a static CI (Figure 11.2).
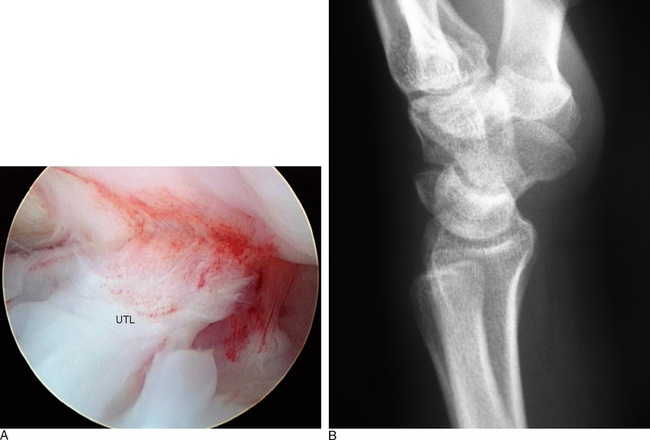
Significant injury to either the ulnocarpal ligamentous complex (ULL and UTL) or the dorsal extrinsic ligaments (DRCL and DICL) will then result in a VISI. Secondary attenuation from prolonged cyclic loading may also play an important role.6,15,17 Although these pathomechanics ultimately result in a VISI type of CID pattern, other carpal instabilities of the nondissociative type [i.e., CIND involving the midcarpal joint (MCJ), radiocarpal joint (RCJ), or combined MCJ/RCJ] can produce similar VISI patterns.13,25
Evaluation of LTJ Injuries
The differential diagnosis of ulnar-sided wrist pain is staggering. Extrinsic wrist disorders and internal wrist derangements must be taken into account during the patient history and physical examination. A careful evaluation of the painful wrist will help to differentiate ulnar-sided pain emanating from LTJ injury versus a variety of associated wrist lesions that mimic ulnar-sided wrist pain. These include TFCC injury, DRUJ injury, MCJ injury and instability, cartilage injury producing chondromalacia and degenerative joint disease, UIS, carpal fractures, dorsal extrinsic ligament sprains, pisotriquetral joint injuries, extensor carpi ulnaris (ECU) subluxation, ulnar neurovascular injuries, and inflammatory connective tissue disorders.13,20,21
A typical patient with an LTIL injury usually presents with a history of acute trauma or repetitive stress to the hand and wrist. Symptoms may be recent or chronic. The ulnar-sided wrist pain is usually intermittent to frequent and is worsened with activities, especially those wrist movements that require rotation and ulnar deviation. Wrist motion produces clicking or a clunk. The wrist feels stiff and the grip is weak. The physical examination usually does not reveal a palmar sag of the carpus (which is characteristic of a VISI) but often shows decreased range of motion, clicking, a clunk with movement, or especially painful ulnar deviation or rotation. There is often tenderness to palpation dorsally at the LTJ region or directly ulnarly over the carpus. Provocative tests that stress the LTJ and reveal pain, crepitus, or joint laxity are suggestive of a ligament injury.26–28
Standard plain posteroanterior and lateral radiographs should be obtained on every patient with a suspected LTJ injury. Typically these radiographs are normal, but they might assist with the differential diagnosis of other wrist injuries known to cause ulnar-sided wrist pain. The plain radiographs can be scrutinized for hints of LTJ instability, such as disruptions of Gilula’s lines, a relative malalignment between the lunate and capitate, or possibly a static collapse with a VISI pattern of lunate flexion and triquetral extension (Figure 11.2B). A gap or diastasis between the lunate and triquetrum is virtually never observed. If a VISI is present, the lunate and capitate are no longer colinear and the lunotriquetral axes become negative (mean value of −16 degrees) whereas the mean value is normally positive at 14 degrees.
Some investigators have advocated wrist motion or stress radiographic studies, cineradiography, three-compartment wrist arthrography, nuclear bone scans, computed tomography, and magnetic resonance imaging (MRI).26,29 The author routinely obtains posteroanterior, lateral, and oblique radiographs of the wrist. In those select patients in whom the diagnosis of wrist pain is still indeterminate, a high-resolution 1.5-Tesla MRI is performed and read by an experienced musculoskeletal radiologist. Even though the MRI scan is neither sensitive nor specific for an LTIL tear, it may produce additional information about other associated wrist joint injuries.
Role of Wrist Arthroscopy
The arthroscopic examination of the painful wrist, especially in the evaluation of LTJ injuries, has become the definitive modality of diagnostic investigation. Wrist arthroscopy is an essential component of a thorough examination because it provides the only direct means of inspecting the integrity of the LTIL, the stability of the LTJ, and the presence of associated wrist joint pathology. Subtle LTJ instabilities that were not detected by the other previously described imaging modalities can now be accurately diagnosed with arthroscopy. Wrist arthroscopy of both the RCJ and the MCJ is now the gold standard in the diagnosis of CI based on its superior accuracy in the direct evaluation of ligamentous injuries.19–28,30–40
Treatment of Lunotriquetral Joint Injuries
In an attempt to minimize the surgical trauma of an open wrist operation and to accelerate the rehabilitation process, the treatment of LTJ instability by arthroscopic technique has been recently investigated.19–28,31–50 The technique of arthroscopic ligament debridement and arthroscopic reduction of LTJ injury with internal fixation using K-wires [i.e., arthroscopic reduction and internal fixation (ARIF)] is described in material following.
In the past, treatment of stable acute and chronic LTJ injuries consisted of a period of splint or cast immobilization in conjunction with other supportive conservative measures.10 It is highly unlikely that this approach will work successfully for any serious acute or chronic LTJ instability. Currently it is believed that only minor acute LTIL sprains respond to rest and immobilization. If symptoms do not improve within six weeks, if the clinical examination is consistent with a moderate or severe sprain of the LTIL, if a wrist MRI scan reveals a serious LTJ injury, or if LTJ instability is already present, arthroscopy should be performed. The degree of LTIL damage, degree of LTJ instability (dynamic or static), and level of associated wrist joint pathology determine whether or not to proceed with ARIF or an open surgical technique.
Direct ligament repair, ligament reconstruction with autogenous tendon graft, LTJ arthrodesis, midcarpal arthrodesis, proximal row carpectomy, and total wrist fusion are the open surgical procedures that have been advocated to restore LTJ alignment and thus the integrity of the PCR. Several investigators have recommended direct ligament repair for an acute injury whenever sufficient LTIL remains.10,26,31,43, The LTIL is reattached to the triquetrum, as this is the usual site of avulsion. The repair technique is surgically demanding, and may require both dorsal and palmar approaches. Augmentation of the LTIL repair with a dorsal capsulodesis to improve the extrinsic ligament support has been suggested to be of some benefit.45–47 The results of direct LTIL repair to restore stability of the LTJ have been satisfactory, with the Mayo Clinic reporting an 86% success rate.31
In patients with chronic static LTJ instability with VISI, or in the case of an arthroscopic or open surgical finding of a nonrepairable LTIL, several investigators have recommended LTIL reconstruction with autogenous tendon graft.10,31,44 On the other hand, other investigators have argued that they prefer an LTJ arthrodesis over a tendon graft reconstruction. The technique of LTIL reconstruction utilizing a distally based strip of extensor or flexor carpi ulnaris is an extremely demanding surgical procedure, and may require significant surgical exposure via dorsal and palmar arthrotomies. Advocates of the reconstruction argue that it preserves LTJ motion and near normal carpal kinematics, as opposed to LTJ arthrodesis that entails significant loss of wrist motion. Only a small group of patients have undergone reconstruction, but the Mayo Clinic group has reported good success.10,31
LTJ arthrodesis is a technically less demanding surgical procedure than reconstruction, and has been shown by several investigators to be successful at reducing or eliminating wrist pain and improving function. It has been reported to have a high rate of LTJ nonunion, however, and mild to slight associated stiffness in wrist mobility.51–55 In several comparative studies of LTJ arthrodesis versus reconstruction or repair, the later groups achieved superior results in regard to patient satisfaction, postoperative complications, and necessity for reoperation.26,31
It should be pointed out that in patients with a fixed VISI deformity it is also necessary to consider reconstruction of the palmar ulnocarpal ligaments or the dorsal extrinsic ligaments in order to prevent permanent rotation of the PCR into a VISI.31,56–58 In some wrists, it may even be necessary to proceed to a midcarpal arthrodesis (i.e., lunate-triquetrum-hamate or lunate-triquetrum-hamate-capitate) if restoration of PCR alignment cannot be achieved.20,45–48,53
Ligamentous repair, reconstruction, or joint arthrodesis needs to take into account the presence of degenerative cartilaginous changes or findings of UIS with degeneration of the TFCC and ulnar cartilage.10,20,21,30,31 In these circumstances, an ulnar shortening osteoplasty may also be needed. As an added benefit from an ulnar shortening, it has been shown that the procedure partially stabilizes the ulnar aspect of the wrist through an increased tension in the ulnocarpal ligament complex.59 Furthermore, a debridement of the degenerative TFCC lesion can be performed. In selected cases, an arthroscopic wafer procedure to remove the protuberant dome of the distal ulna might be feasible in place of an ulnar shortening osteotomy.59,60
Arthroscopic Technique
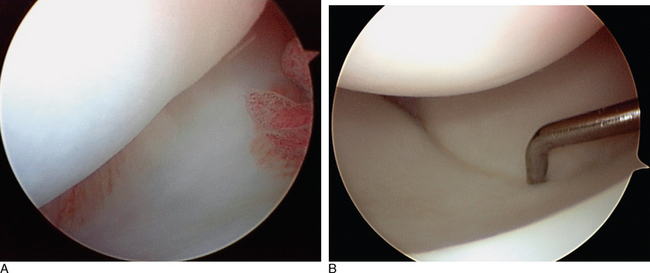
The ulnocarpal ligaments (ULL and UTL) are clearly seen, as is the entire TFCC and the cartilaginous surfaces of the entire PCR (Figure 11.3). The volar portion of the LTIL is best visualized through the ulnar (6-U) portal, where it can be seen in its entirety (Figure 11.1C). As an alternative, a volar wrist portal can be established that also provides excellent viewing of the volar LTIL and dorsal wrist structures such as the DRCL (Figure 11.4B). Associated injuries to the TFCC, extrinsic ligaments, cartilage, and capsule can be assessed with RCJ arthroscopy using a combination of these four portals.
< div class='tao-gold-member'>
Related posts:
 Arthroscopy of the Distal Radioulnar Joint
Arthroscopy of the Distal Radioulnar Joint
 Arthroscopic Plication of Lunotriquetral Ligament Tears
Arthroscopic Plication of Lunotriquetral Ligament Tears
 Arthroscopic Treatment of Scapholunate Ligament Tears
Arthroscopic Treatment of Scapholunate Ligament Tears
 Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
 Arthroscopically Assisted Reduction and Percutaneous Fixation of Scaphoid Fractures Using a Simple External Targeting System
Arthroscopically Assisted Reduction and Percutaneous Fixation of Scaphoid Fractures Using a Simple External Targeting System
 Wrist Arthroscopy Portals
Wrist Arthroscopy Portals
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


