Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Marc Safran
Michael Kalisvaart
DEFINITION
Osteochondritis dissecans (OCD) is a progressive form of osteochondrosis involving focal injury to the subchondral bone or its blood supply. It may occur in many different areas of the adolescent skeleton.
The knee is the most common location for OCD, but it may occur in several locations of the elbow, including the radial head, the trochlea, and the capitellum (the most common location within the elbow).
The injury to the subchondral bone results in loss of structural support for the overlying articular cartilage. As a result, degeneration and fragmentation of the articular cartilage and underlying bone occur, often with the formation of loose bodies.
The histopathology of the subchondral bone in OCD is consistent with osteonecrosis.
Articular cartilage injury may also occur anywhere in the elbow, especially after trauma. More common locations of nonarthritic chondral injury include the radial head and capitellum.
ANATOMY
Bony Anatomy
The bony anatomy of the elbow allows for two complex motions: flexion-extension and pronation-supination.
The ulnohumeral articulation of the elbow is almost a true hinge joint with its constant axis of rotation through the lateral epicondyle and just anterior and inferior to the medial epicondyle. This well-fitted hinge joint allows for little excessive motion or toggle.

FIG 1 • A. Cross-section of the elbow showing the round, convex capitellum and the matching concave radial head. B. Anatomy of the medial elbow ligamentous complex. The ulnar collateral ligament complex comprises three ligaments: the anterior oblique, posterior oblique, and transverse ligaments.
The radius articulates with the proximal ulna and rounded capitellum of the distal humerus. The radiocapitellar joint and the proximal radioulnar joint allow for pronation-supination (FIG 1A). The ulnohumeral joint allows for flexion-extension of the elbow.
The ulnohumeral joint has 11 to 16 degrees of valgus. This results in increased compressive force in the lateral elbow (radiocapitellar joint) with axial loading.
Ligamentous Anatomy
The ligaments of the elbow are divided into the radial and ulnar collateral ligament complexes.
The lateral or radial collateral ligamentous complex provides varus stability. These ligaments are rarely stressed in the athlete.
The ulnar or medial collateral ligament complex consists of three ligaments: the anterior oblique, the posterior oblique, and the transverse.
The ulnar collateral ligament complex, particularly the anterior oblique ligament, resists valgus force, such as occurs with throwing, whereas the radiocapitellar joint is a secondary restraint to valgus force (FIG 1B).
Intraosseous Vascular Anatomy
There are two nutrient vessels in the lateral condyle of the developing elbow.
Each vessel extends into the lateral aspect of the trochlea, with one entering proximal to the articular cartilage and the other entering posterolaterally at the origin of the capsule.
Although these two vessels communicate with each other, they do not do so with the metaphyseal vasculature. The rapidly expanding capitellar epiphysis in the developing elbow thus receives its blood supply from one or two isolated transchondroepiphyseal vessels that enter the epiphysis posteriorly.
These vessels function as end arteries passing through the cartilaginous epiphysis to the capitellum.
Metaphyseal vascular anastomoses do not make significant contributions to the capitellum until approximately 19 years of age, placing this region at risk for vascular injury.
PATHOGENESIS
The cause of OCD is unclear and controversial.
OCD typically affects the dominant extremity of adolescents and young adults, with onset of symptoms between 11 and 16 years of age.
Most cases are seen in high-level athletes who experience repetitive valgus stress and lateral compression across the elbow (eg, overhead-throwing athletes, gymnasts, weightlifters).
The lesion usually affects only a portion of the capitellum.
Genetic factors, trauma, and ischemia have been proposed as causes.
Most authors believe that the primary mechanism of injury is repetitive microtrauma in a genetically predisposed individual’s developing elbow that results in vascular injury due to the tenuous blood supply.
The capitellum is softer than the radial head.
Repeated microtrauma, such as axial loading in the extended elbow or repeated throwing that produces valgus forces on the elbow, results in increased force in the radiocapitellar joint.
The repetitive microtrauma caused by these forces has been proposed to weaken the capitellar subchondral bone and result in fatigue fracture.
Should failure of bony repair occur, an avascular portion of bone may then undergo resorption with further weakening of the subchondral architecture. This is consistent with the characteristic rarefaction often seen at the periphery of the lesion.
The altered subchondral architecture can no longer support the overlying articular cartilage, rendering it vulnerable to shear stresses, which may lead to fragmentation.
The tenuous blood supply of the end arterioles in the capitellum may become injured with the repetitive microtrauma, resulting in OCD.
Although a genetic predisposition to OCD has been proposed in the literature, convincing scientific evidence of OCD as a heritable condition does not currently exist. Some individuals are more susceptible than others, and this may be genetically based.
NATURAL HISTORY
The natural history of capitellar OCD is unpredictable. No reliable criteria exist for predicting which lesions will collapse with subsequent joint incongruity and which will go on to heal without further sequelae.
If healing is going to take place, it usually occurs by the time of physeal closure.
If healing is not going to take place, repetitive microtrauma and shear stresses to the articular surface of a lesion that has lost its subchondral support may result in further subchondral collapse and deformation with joint incongruity as well as articular cartilage injury, fragmentation, and loose body formation.
In advanced cases, degenerative changes accompanied by a decreased range of motion are likely to develop.
PATIENT HISTORY AND PHYSICAL FINDINGS
The classic patient with OCD is an adolescent athlete who experiences repetitive valgus stress and lateral compression across the elbow (eg, overhead-throwing athletes, gymnasts, weightlifters).
The patient usually complains of the insidious onset of poorly localized, progressive lateral elbow pain in the dominant arm.
He or she may also note a flexion contracture.
The throwing athlete may note a reduction in throwing distance or velocity or both.
Prodromal pain is not always present.
Typically, pain is exacerbated with activity and relieved by rest.
In advanced cases in which a fragment has become unstable or loose body formation has occurred, mechanical symptoms of elbow locking, clicking, or catching may be present.
Physical examination methods
On examination, there may be tenderness to palpation and crepitus over the radiocapitellar joint.
Effusion indicates intra-articular irritation and may be consistent with a loose or unstable OCD lesion or loose body.
Swelling, palpated in the posterolateral gutter (soft spot), may be appreciated.
Crepitus may be present on range-of-motion testing.
Loss of 10 to 20 degrees of extension is common, and mild loss of flexion and forearm rotation may also be seen. Loss of pronation is less common.
Provocative testing includes the “active radiocapitellar compression test,” which consists of forearm pronation and supination with the elbow in full extension in an attempt to reproduce symptoms.
The examiner should rule out radiocapitellar overload as the result of ulnar collateral ligament insufficiency using the milking maneuver, modified milking maneuver, valgus stress test, or moving valgus stress test.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Diagnostic evaluation of the elbow for OCD begins with plain radiographs—an anteroposterior (AP) view, lateral view, oblique views, and a 45-degree flexion AP view, which is particularly good at revealing the lesion.
Radiographs typically show the classic radiolucency (FIG 2A) or rarefaction of the capitellum (FIG 2B) in addition to irregularity or flattening of the articular surface.
The lesion frequently appears as a focal rim of sclerotic bone surrounding a radiolucent crater with rarefaction located in the anterolateral aspect of the capitellum.
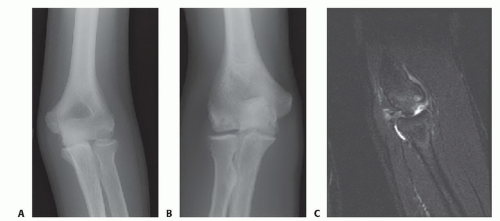
FIG 2 • A. Radiograph of a 15-year-old baseball pitcher with OCD of the capitellum of the dominant elbow. Clear lesion and sclerosis of the bony bed are shown. B. OCD in a 15-year-old gymnast with rarefaction of the capitellar lesion on oblique radiograph of the elbow. C. MRI of the elbow of a baseball pitcher, revealing OCD with loss of overlying articular cartilage and loose body.
Radiographs, however, may not reveal the osteochondral lesions in the earlier stages. They are not of much benefit for truly chondral lesions.
In advanced cases, articular surface collapse, loose bodies, subchondral cysts, radial head enlargement, and osteophyte formation may be seen.
Further diagnostic imaging of OCD lesions primarily consists of magnetic resonance imaging (MRI), although ultrasonography and bone scintigraphy have been used.
MRI is especially valuable in assessing the integrity of the articular cartilage overlying the OCD lesion as well as in diagnosing OCD in its early stages and identifying loose bodies (FIG 2C).
Controversy exists over the use of contrast-enhanced magnetic resonance arthrography. This technique, however, can potentially provide additional information regarding the status of the articular cartilage and identification of loose bodies.
Bone scintigraphy is very sensitive for identifying osteoblastic activity or increased vascularity at the site of an OCD lesion. However, it is nonspecific and has limited usefulness in diagnosis.
Computed tomography can help define bony anatomy and identify loose bodies.
Ultrasonography can also help in the assessment of capitellar lesions, including early stages, but ultrasound is technician dependent.
DIFFERENTIAL DIAGNOSIS
Panner disease
Infection
Lateral epicondylosis
Lateral epicondylar apophysitis
Radial head osteochondrosis
Radial head or neck injury
Radiocapitellar overload and chondromalacia due to ulnar collateral ligament injury
Posterolateral rotatory instability
NONOPERATIVE MANAGEMENT
The choice of conservative or surgical management depends on the patient’s age, symptoms, size of the lesion, and stage of the lesion, specifically the integrity of the cartilage surface.
The goal of treatment for OCD of the elbow is to prevent the progression of the disorder, detachment of the osteochondral lesion, and degenerative changes of the articular cartilage.
Small, nondisplaced lesions with intact overlying articular cartilage in younger (skeletally immature) athletes are best managed conservatively with relative rest and activity modification, ice, and nonsteroidal anti-inflammatories, particularly if the bone scan shows increased bony activity.
Activity modification consists of avoiding throwing activities and weight bearing on the involved arm.
Short-term immobilization (less than 2 to 3 weeks, depending on symptoms) may be considered.
Serial radiographs, at 10- to 12-week intervals, are obtained to monitor healing.
Activity modification is continued until the radiographic appearance of revascularization and healing.
Radiographic findings of OCD may persist for several years. As a result, after conservative management, the most important issue in terms of an athlete’s ability to return to sports is symptom resolution.
Most patients can return to full activity after 6 months.
SURGICAL MANAGEMENT
The indications for surgical treatment include persistent symptoms despite conservative management, symptomatic loose bodies, articular cartilage fracture, displacement of the osteochondral lesion, and cold bone scan.
The surgeon must assess the size, stability, and viability of the fragment and decide whether to remove the fragment or attempt to surgically reattach it.
Most fragments cannot be reattached and therefore are excised, followed by local débridement.
Arthroscopic abrasion chondroplasty or subchondral drilling may be performed to encourage healing.
Although symptoms usually improve, about half of all patients will continue to have chronic pain or limited range of motion.
In general, many athletes cannot return to their prior levels of competition.
Surgical indications for operative management of stable lesions with intact articular cartilage include radiographic evidence of lesion progression and failure of symptom resolution despite a 6-month trial of a conservative, nonoperative regimen.
Arthroscopic examination, débridement as needed, and drilling or microfracture of the OCD lesion (with or without in situ pinning) are usually the surgical treatments of choice.
Unstable lesions, characterized by overlying articular cartilage injury and instability as well as collapse or disruption of the subchondral bone architecture, and those with loose bodies are usually managed surgically.
These lesions are frequently flap lesions. They characteristically present with more advanced radiographic changes (including a well-demarcated fragment surrounded by a sclerotic margin).

FIG 3 • A. Lateral positioning for elbow arthroscopy, including tourniquet placement. B. Setup in the operating room for the lateral position. C. Prone position of the patient. This is the preferred position, particularly due to the ease of posterior elbow access. The setup of the room is the same and the relative position of the elbow for the surgeon is similar between the prone and lateral positions. D. Supine position of the patient. Some surgeons prefer this position because it is easier to convert to open surgery and easier anesthesia management; however, posterior arthroscopic access is more difficult in this position.
There is controversy whether simple fragment excision or reduction (open or arthroscopic) and internal fixation is the preferred treatment. Many authors advocate excision of displaced fragments, often augmented by drilling or microfracture.
Critical considerations in operative planning include the size and integrity (viability) of the fragment, the subchondral architecture on the fragment and the opposing bony bed, the potential for anatomic restoration of the articular surface, and the method of fixation if attempted.
Internal fixation of the fragment may be performed using metallic screws, bioabsorbable screws or pins, Kirschner wire, bone pegs, and dynamic staple fixation.Related posts:
 Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Posterior Shoulder Instability
 Glenoid Bone Graft for Instability with Bone Loss
Glenoid Bone Graft for Instability with Bone Loss
 Athletic Pubalgia and Adductor Injuries
Athletic Pubalgia and Adductor Injuries
 Repair of Acute and Chronic Patella Tendon Tears
Repair of Acute and Chronic Patella Tendon Tears
 Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
Anterior Cruciate Ligament Reconstruction in the Skeletally Immature Patient
 Modified Brostrom and Brostrom-Evans Procedures
Modified Brostrom and Brostrom-Evans Procedures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


