CHAPTER 10 Arthroscopic Thermal Shrinkage for Scapholunate Ligament Injuries
Introduction
The use of arthroscopic thermal shrinkage with radiofrequency (RF) for the treatment of scapholunate (SL) ligament injuries is a recent technique, but the real effectiveness is undetermined.1–3 The ability of RF probes to both debride and shrink tissues makes them an attractive alternative to the use of a mechanized resector for debridement of SL ligament tears, and provides a means of stabilizing the SL joint.
What Is Shrinkage?
Shrinkage is a physical phenomenon that occurs with heat modification of type I collagen in ligamentous tissue. When the collagen is heated to a critical temperature, the heat-labile intramolecular hydrogen bonds break.4 The protein undergoes a phase transition from a highly ordered crystalline structure to a random-coil state (similar to a melted state) and the tissue tensile properties change.5 Typically, this thermal denaturation of collagen type I occurs at approximately 60 to 65° C.
Molecular Effects of Thermal Shrinkage
Transmission electron microscopy shows significant alterations in the collagen architecture. These changes are characterized by the loss of the classic 67-nm periodicity of the type I collagen fibril that is evidenced by the loss of the periodical cross-striations in the collagen fibril. There is also an increase in the cross-sectional area of the collagen fibril. The margins of the fibrils begin to lose their distinct edge, while maintaining their circular shape. These ultrastructural effects are caused by unwinding of the collagen triple-helix as a result of the temperature rise in the tissue.6,7
Biologic Response to Thermal Shrinkage
At time 0, after thermal shrinkage there is evidence under light microscopy of diffuse hyalinization and fusion of the collagen fiber. By day 7, there is fibroblast proliferation around and within the hyalinized regions. By day 30, large fibroblasts have migrated into the region and have produced a new matrix. These newly arrived fibroblasts use the acellular “hyalinized” collagen as a scaffold for migration and matrix synthesis. At three months, active reparative changes are evident (with an increase in vascularity). The fibroblasts have now regained a more normal appearance under transmission electron microscopy. At seven months, cell morphology and vascularity have returned to normal—without evidence of permanent tissue injury or severe inflammation.8,9
Biomechanical Effects of Thermal Shrinkage
Experimental studies have shown that (1) ligaments and joint capsular tissue can be modified significantly (shortened) by thermal energy at the temperature range of 70 to 80° C, (2) thermal energy causes immediate deleterious effects such as loss of the mechanical properties, collagen denaturation, and cell necrosis, (3) thermally treated tissue is repaired actively by a residual population of fibroblasts and vascular cells, with concomitant improvement of mechanical properties, (4) the shrunken tissue stretches with time if the tissue is subjected to physiologic loading immediately after surgery, and (5) leaving viable tissue between treated regions significantly improves the healing process.10,11
Rationale for Shrinkage of Scapholunate Ligament Injuries
Our concept for the use of thermal shrinkage for the treatment of instability of the carpus with scapholunate ligament injuries arose from previous published work on the use of thermal shrinkage on other articulations, as well as the favorable results that were achieved following mechanical debridement of partial SL ligament tears.12,13 We were also influenced by the biomechanical importance of the SL ligament for stability of the carpus and the paucity of treatment methods for carpal instability, as well as the relative ease of performing an arthroscopic shrinkage of the SL ligament.
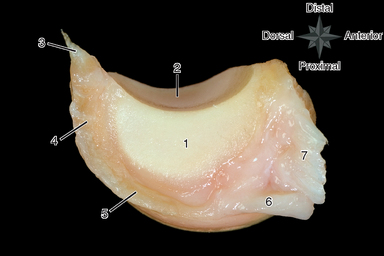
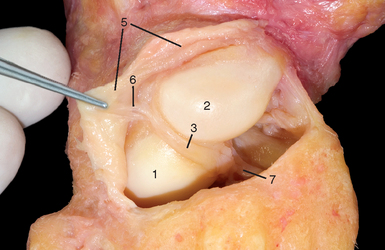
The SL ligament is not a homogeneous structure. It is divided into three parts: dorsal, proximal, and palmar (Figure 10.1). The dorsal part is the strongest subregion of the SL ligament. It meets all criteria for the definition of an articular ligament in that it is composed of collagen fascicles surrounded by connective tissue with intertwined neurovascular bundles.14–16 It has a thickness of 2 to 3 mm and a length of 4 to 5 mm (Figure 10.2), and it merges with the dorsal capsule (Figure 10.3).

The proximal portion is grossly anisotropic. It is composed mainly of fibrocartilaginous tissue, which is relatively weak due to its avascularity. The transition zone between the proximal and palmar portions is marked by the radioscapholunate ligament, which inserts on the palmar aspect of the scapholunate ligament. The palmar portion is composed of thin collagen fascicles (1 mm thick) of length 4 to 5 mm. This portion is not visible through the standard dorsal arthroscopic portals in the face of an intact radioscapholunate ligament.
The three parts do not have the same tensile strength. The dorsal part is most resistant to shear forces, with an ultimate yield strength of 300 N. The palmar part fails at a load of 150 N, whereas the proximal portion can withstand only 25 to 50 N of stress. The triquetrolunate ligament, which is also divided into three parts, has the exact reverse characteristics in regard to loading failure as those of the SL ligament. Biomechanical studies have also demonstrated that the dorsal subregion of the SL ligament is responsible for controlling scaphoid flexion and the extension motion, whereas the palmar subregion controls rotational motion.17–20
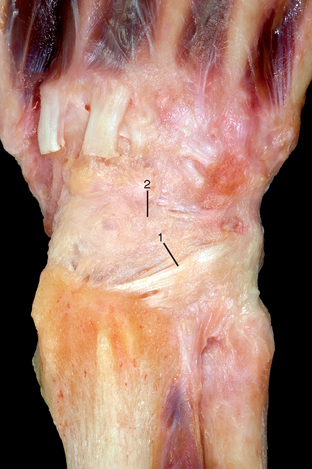
Based on this evidence, it was apparent to us that the use of thermal shrinkage of the SL ligament was feasible and most appropriate for the dorsal part of the ligament. When considering the kinematics and the instability of the carpus in SL ligament injuries, it is important to remember the role of the dorsal radiocarpal ligaments (Figure 10.4) and the dorsal capsule (Figure 10.5). They are initimately connected with the SL ligament and must be included in the thermal shrinkage (Figure 10.6).
< div class='tao-gold-member'>
Related posts:
 Arthroscopy of the Distal Radioulnar Joint
Arthroscopy of the Distal Radioulnar Joint
 Arthroscopic Plication of Lunotriquetral Ligament Tears
Arthroscopic Plication of Lunotriquetral Ligament Tears
 Arthroscopic Treatment of Scapholunate Ligament Tears
Arthroscopic Treatment of Scapholunate Ligament Tears
 Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
 Wrist Arthroscopy Portals
Wrist Arthroscopy Portals
 Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


