Arthroscopic Subacromial Decompression and Distal Clavicle Resection
Patient Selection
Subacromial impingement and degenerative changes of the acromioclavicular joint are common causes of shoulder pain; they often result from repetitive overhead use that leads to inflammation of the bursa and supraspinatus tendon as they pass under the acromion
Pain reported with overhead activities, lateral shoulder pain, night pain, and pain with abduction and internal rotation
Surgical intervention is indicated following failure of a 3- to 6-month course of nonsurgical management that includes anti-inflammatory medications, physical therapy with rotator cuff strengthening, and activity modification
Preoperative Imaging
Radiography
True AP view of the glenohumeral joint
Outlet view to evaluate the acromion
Axillary lateral view to rule out os acromiale
Zanca view to evaluate acromioclavicular joint
Magnetic Resonance Imaging
Helpful in assessing condition of rotator cuff
Increased signal intensity at acromioclavicular joint can aid in confirming the diagnosis
 | Video 24.1 Subacromial Decompression and Distal Clavicle Resection. Mark Rodosky, MD; Albert Lin, MD (6 min) |
Procedure
Room Setup/Patient Positioning
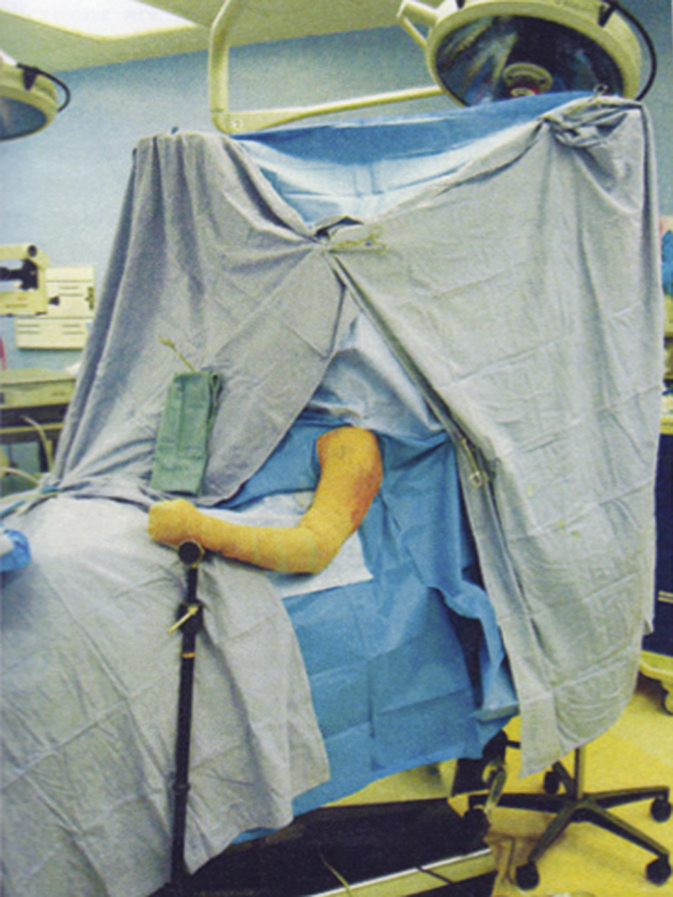
Figure 1Photograph demonstrates upright beach-chair positioning of a patient for arthroscopic subacromial decompression and distal clavicle resection.
Upright in beach-chair position (Figure 1)
Acromion parallel to the floor
Bony prominences well padded
Special Instruments/Equipment/Implants
30° arthroscope
4.5- and 5.5-mm arthroscopic shavers
5.5-mm arthroscopic burr
Standard and hooked arthroscopic electrocautery devices
Surgical Technique
Examination Under Anesthesia
Should be performed to evaluate range of motion (ROM) and ligamentous laxity
Side-to-side comparison with nonsurgical limb can be done
Landmarks/Portals
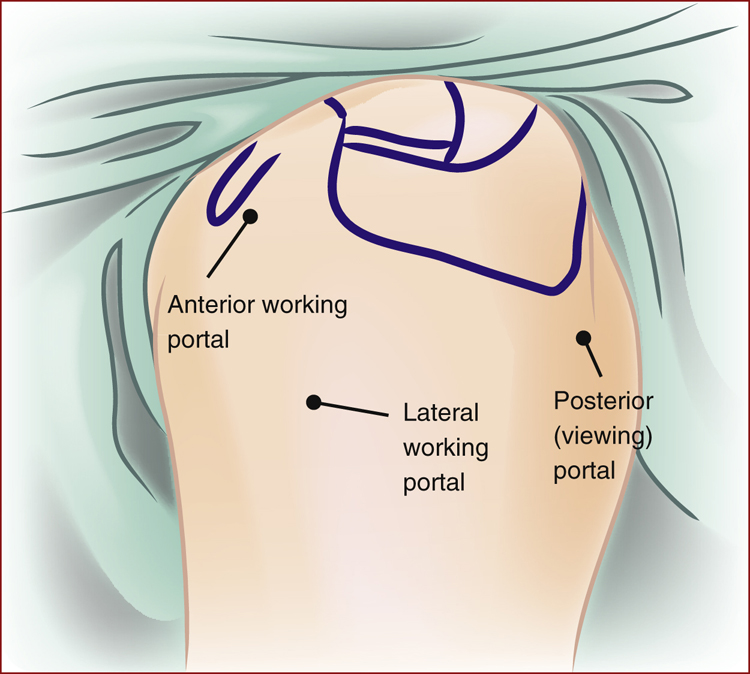
Figure 2Illustration of a left shoulder shows the location of the anterior working portal, lateral working portal, and posterior (viewing) portal in relationship to the coracoid, clavicle, acromion, and scapular spine, which are marked on the skin.
Mark arthroscopic portal sites and other bony landmarks (Figure 2)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


